She's pretty, and sweet. I've ordered a DNA test for her.
There’s an old Chinese parable that goes something like this:
A farmer gets a horse, which soon runs away. A neighbor says, “Oh, so sorry for the bad news.” The farmer replies, “Good news, bad news, who can say?”
The horse comes back and brings another horse with him. Good news, perhaps.
The farmer gives the second horse to his son, who rides it, then is thrown and badly breaks his leg. Ack! Bad news! “Well,” says the farmer. “Who can say?”
A few days later, the emperor’s men come and take every able-bodied young man to fight in a war. The farmer’s son is spared. So, good news!
The message of the story: “Good news, bad news, who can say?” We can never know ahead of time how things that may appear to be good or bad will turn out.
I’m thinking about this at the moment, because I am fostering a puppy with a “Good news, bad news, who can say?” sort of back story.
As I’ve written about before, I’ve been volunteering at the emergency shelter being provided to evacuees of the North Complex Fire, one of many that erupted in California following a dry lightning storm on August 17. My local animal rescue group, the North Valley Animal Disaster Group, opened the shelter on September 8, when a windstorm pushed the North Complex fire 30 miles overnight and right into our backyard (10 miles from my literal backyard). And an army of volunteers have been caring for hundreds of dogs, cats, birds, rabbits, horses, sheep, goats, pigs, llamas, donkeys, chickens, ducks, you name it ever since.
I was evacuated for a few days, myself. When my husband and I (and our dogs, of course) were allowed to go home, the first thing I did was report for duty at the shelter to walk and feed dogs.
The emergency shelter is a temporary facility; dogs are kept in crates, so they HAVE to be walked multiple times a day. Not an easy task, when they are in close quarters, the air is full of smoke, there are dozens of strangers walking among them, their crates are packed close together next to those of other stressed dogs … It’s a very tough situation.
On my first day of volunteering, I was assigned to work in two rooms at the shelter – which is located in a series of rooms in the bowels of a former county hospital. (One of the rooms used to be the county morgue! The building stopped being a hospital sometime in the early 1970s.) One of the rooms I was overseeing was the “isolation” room, where puppies who were likely to be as-yet unvaccinated were being kept. Among them were three pups who appeared to be siblings, about 5 months old. (Hey! Good news! Their owner evacuated the fire zone and brought them to an appropriate place for care!)
All three of these puppies were terrified of people and of being held in the crates. One, who appeared to be the runt of the litter, would shyly wag his tail at people, but the other two didn’t want to make eye contact and avoided touch. And one, the only female, appeared to have something very wrong with her back end; she was limping or crippled or something. (Yikes, bad news, right?) Hard to tell in the crate. They were going to be especially challenging to care for.
A day later, I learned that the female pup had been placed under a 10-day quarantine. She had bitten one of the volunteers who was trying to get her out of her crate for a walk. Terrible news, right?
A mystery condition: what’s wrong with her back legs?
The county animal control officer overseeing the shelter contacted her owner, informing him of both the bite and quarantine, and also informing him that the pup needed to be transported to a veterinarian for medical care; what was going on with her rear legs? Citing the difficulties of his situation (I believe his home was burned in the fire), the owner relinquished her to the county. (Bad news? No, actually, good news! The county can pay for her to be seen by a veterinarian!)
“Coco,” as she is now known to be named, was transported to a local veterinarian. She was so incredibly scared, the examination was rather perfunctory. A soft-tissue injury was suspected, pain meds were prescribed to see if they help, and she was sent to the local permanent shelter to serve out the rest of her quarantine. Hard time! Bad news?
Well, no: Upon intake to the permanent shelter, she was vaccinated, like all “stray” dogs and dogs who are relinquished to the city or county by their owners. A week later, at the emergency shelter, it was reported that seven owned dogs who were being cared for at the emergency shelter had developed parvovirus. Oh my gosh, this is terrible news for those dogs – and I didn’t yet know whether it was Coco’s brothers who were infected, or some other dogs, because I hadn’t been to the shelter in the past week (busy getting the November issue of WDJ to the printer) – but being sent to the permanent shelter was great news for Coco, who got to miss being exposed to parvo, and who received the benefit of what may have even been her first vaccination.
I was keeping track of Coco’s incarceration, because I made it known that I would be happy to foster her when she was released from her quarantine; I knew she needed further medical care, to see what was going on with her back end, and was afraid she’d get lost in the shuffle. It just seemed to me that she had gotten a really poor hand of cards so far in life. Following her last day in quarantine, I started pushing the animal control officer in charge of her case for information about her vet care, and asked if I could foster her. Happily, the officer agreed that we couldn’t know for sure what was ailing the puppy unless she had x-rays taken, so he made an appointment to go back to the vet and I volunteered to transport her.
Coco on her way home from the shelter and the vet’s office.
After 10 days in a kennel at the shelter, she was both more habituated to loud, barky surroundings and seeing people. She still looked tense and scared, but the shelter vet tech was able to pick her up and carry her to my car without having to put a muzzle on her. At the vet’s office, of course, they did put a muzzle on her, so they could safely sedate her for x-rays.
The radiographs came back without offering a single clue as to the source of her problem: Spine fine, hips fine, pelvis fine, knees fine. Good news?
At this point, it must be said, nobody had been able to see Coco move about freely, to really study exactly what was wrong with her. As she moved around in a crate or kennel, always trying to avoid contact with humans, all you could tell was that she couldn’t really stand up or walk properly.
Woody to the rescue once again
So, I brought her home! In the car, I put a soft, padded harness on her – carefully, gently –and attached a long line to it. I own two fenced acres and two dogs who are experienced with foster puppies and strange dogs.
It took about an hour for my five-year-old “fun uncle” dog, Woody, to convince her that no one was going to try to murder her at our house. It took only another hour and many Stella and Chewy’s freeze dried chicken Meal Mixers (my dog training secret weapon) to convince her that I was safe, she didn’t want to go anywhere (I could take off the harness), and that Woody was her absolute crush. I mean, honestly. It’s a little embarrassing.
“I might survive if I can be near you, Woody!”
Over this past week, while I’ve been tied to my home office and computer, Coco has gone from terrified to terrific – at least as far as being comfortable with humans is concerned. (She likely was fine with her original human family, but the abrupt move under emergency conditions into a crate in a crowded facility just blew her little mind.)
And all this week, I’ve been taking pictures and video of Coco on the move. Good news, bad news, who knows? It’s a mystery.
She certainly can move; she can run and jump and go up and down stairs – but her rear end doesn’t move right – I mean, properly. She hops like a bunny behind; both hind legs move as one: hop, hop, hop. She does not – can not? – move her back legs independently of each other. If you hold a treat in front of her nose and try to get her to move forward just one leg at a time, she will step, step with her front feet, and streeeeettttchhh with her back feet, and then hop with both. If you hold one of those back legs (gently) to see if she will step with the other one, she just falls down.
I really, really wanted to see what Coco would do in water. Would the non-weight-bearing environment make her comfortable enough to move her legs in a normal movement pattern? Would her brain be “reset” by the need to swim into paddling her back legs independently? A friend and I took her to a local reservoir that has a shallow, soft bottom. I carried her out to a depth where her feet could just barely brush the ground, supporting her with one hand under her chest and feeling with the other hand under water to see what her hind legs would do.
They paddled independently.
This made me so happy. There is hope! She is happy, she is able, she is not in pain … She is not right, but there is hope for her.
They sleep like this daily.
I got an unofficial consult from a friend who is also a NVADG volunteer (except she’s a BEAST on the animal evacuation team, who goes into the fire zone rescuing animals) and an equine massage therapist when our county is not on fire. Tamara came to my house and met Coco, watching her hop and run and play with Woody. She also massaged and stretched the little dog, and she agrees: Coco’s condition is weird, but there’s hope. We both think Coco needs more swimming time, and time on an underwater treadmill. Acupuncture? Massage? Stretching? Physical therapy? We think she needs all of it.
So, sorry, Otto, we’ve got one more project puppy we need to help. Though, frankly, if I can find an underwater treadmill and a PT specialist to help me with Coco, I will sign up Otto for therapy, too! At 13 years old, he would benefit from this sort of care just as much as I think Coco will.
Now 13 years old, Otto’s body looks thicker than it did when he was younger, but he’s lost muscle mass, especially in his hind legs and shoulders. His fuzzy coat makes him look stocky, but his ribs and spine are actually more prominent than in years past.
Over the past two years, my senior dog, Otto, has started having trouble maintaining his body mass at a healthy weight. He has had a few health issues that his veterinarians and I are monitoring, but one symptom of his issues has caused him to suffer from a bit of gastric reflux. We have been able to keep his stomach acid in check with a daily medication, but there was a period of months when he just didn’t feel like eating. During that time, I had to tempt his appetite with all sorts of foods, split into many small meals a day, to get him to eat at all. At his lowest, his weight, normally about 70 pounds, dipped all the way down to 63 pounds. He felt ribby and definitely lost muscle mass.
Eventually, the tide turned and Otto started eating again, although it was a challenge to get him back up to his “college” weight of 70 pounds. I can’t give him huge meals – he won’t eat a ton in one sitting – so I often give him three meals a day. He also gets canned food mixed into his dry food at each meal, and eats more than a can a day. I also mix some warm water into his food and stir the canned food in, so he doesn’t pick out the canned food and leave any kibble behind.
One unfortunate side effect of the campaign to get Otto to gain and hold his weight: My younger dog Woody has gained too much weight! Because when he sees the canned food come out, he (quite understandably) wants some, too. I don’t have to, of course, but I stir about a teaspoonful of the canned food into Woody’s kibble, and add warm water to it, so he feels like he’s getting special treatment, too. So, of course, I’ve had to cut back the amount of kibble he gets, just a little bit, to make up for the addition of the fattier canned food.
At age 5, Woody is in the prime of his life. He is carrying a few more pounds than I would like, even though it is hard to see given his deep chest and narrow waist. But his ribs are more padded than what is ideal. He is such an active dog that carrying extra weight stresses his joints more than is good for him.
It’s nuts: Both dogs used to weigh the same amount. To get and keep Otto at 70 pounds, I’ve added nearly an entire can of food to what he gets each day, and have had to reduce Woody’s portion of dry food to make up for the addition of only a teaspoon of canned food, and yet Woody is up to about 73 or 74 pounds.
It’s hard to get two dogs to stand with their backs to you while you hover over them, but I did my best. As you can see, both dogs look okay – but Otto’s waist is a bit more pronounced, and Woody’s is less defined than ever before.
I know it’s silly to feel as though Woody would judge me for failing to add anything “nice” to his kibble at each meal, and yet, I absolutely see him watching me carefully when I prepare both dogs’ meals. I actually fork the wet food from the cans into the dogs’ bowls with my back blocking his view, so he can’t see how much of the delicious pâté goes into each bowl, and I deliver the food to them separately. Otto eats outside, with his bowl on a stair that’s one step higher than the deck; Woody eats in the house.
Another wrinkle: Since Coronavirus has changed the world, we definitely have been going out less. The lack of walks has likely contributed both to Otto’s loss of muscle mass and Woody’s weight gain.
Also, I give Otto a pill each day hidden in a piece of cheese. Woody, too, lines up and sits politely, looking for his cheese. Those extra calories, too, aren’t helping me maintain his figure!
Have you had this problem before? Trying to keep one dog thin and helping another dog gain weight? Do you have any tips for us?
There are so many food choices available to dog owners today; it's easy to get overwhelmed. But whatever you do, don't just feed the same thing month in and month out; rotating foods from different manufacturers helps provide your dog with nutritional balance over time. It also reduces the potential danger of any pet food company's formulation error or production problem.
Were you aware that dogs don’t have a biological requirement for carbohydrates? The fact that this bit of trivia sounds so crazy is a testament to how thoroughly we all take carbohydrate-laden kibble for granted. But it’s true: Dogs require protein and fat, but they can live and thrive quite well without any carbs at all.
Perhaps you’ve seen canned foods with labels indicating that meat makes up 93% or 95% (or sometimes even 96%!) of the product. This is possible because nearly all of a dog’s nutritional requirements can be met in a diet mainly comprised of meat; add some vitamins and minerals, and he’s all set!
But dogs can eat and benefit from carbohydrates – and the foods that provide carbs are much less costly than the foods that provide just protein and fat, so pet food makers can provide adequate nutrition to dogs for a lower price by using a certain amount of carbohydrate-based ingredients in their food. Generally, the more carbs there are in the can, the less the food will cost.
Cost isn’t the only reason to add a non-meat ingredient to a diet for dogs, however. Some ingredients provide non-nutritive functions that benefit the dog. For example, some fruits, vegetables, grains, and legumes provide fiber that can modify or improve the dog’s intestinal microflora, so he can better digest his food. Some foods can reduce inflammation or provide antioxidant action. Certain herbs and spices have been shown to improve mobility or cognition.
All of the “complete and balanced” foods you can buy for your dog will meet his requirements – whether his requirements are just for the basic maintenance of life or the higher nutritional needs of a growing puppy. But, as you’ll see, each pet food maker will approach the task of meeting those needs in any number of ways, with any number of ingredients.
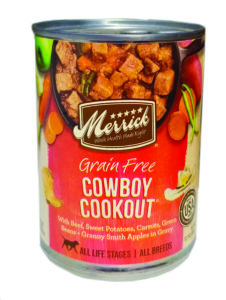
Test Your Label Reading Skills!
What’s important on the label – and what’s inconsequential?
Pay attention to:
• Name of pet food company
• What dogs the food is formulated for (note that this is not the complete, legal nutritional adequacy statement, but it is nice to have the information up front)
Disregard entirely:
• Pretty pictures of fresh vegetables
• Ingredients called out on the front of the can (they are just there to tempt your own appetite; the position on the legal ingredient list may be very different)
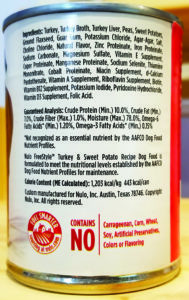
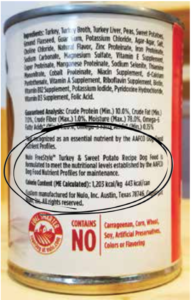
Pay attention to:
• Ingredient list, at least to the 10th or so ingredient. Once you reach the salt on a label, the amounts of the ingredients are vanishingly small
(so don’t get too excited about foods, herbs, or nutraceuticals that appear low on the ingredient list)
• Guaranteed analysis: There are consequences for pet food makers if the product does not deliver these theamounts of any nutrients that are present here. The minimum amount of protein and fat, and maximum amount of fiber and moisture must appear here. Anything else included here is optional.
• Calorie content. Helpful if you are not as familiar with the fat and protein content.
• Location information for the manufacturer must appear on the label. A phone number is not required by law but c’mon! One should be present.
Disregard entirely:
• Verbiage about what the food does NOT contain.
YOU CAN DO THIS
Your task is to find foods that “perform well” in your dog – that improve or maintain his digestion (helping build a nice stool, not too hard and not too soft, and reducing or eliminating excessive gas); maintain or improve his health, appetite, and energy; and, if he’s a puppy, provide for an appropriate rate of growth (not too fast, not too slow).
How the heck are you supposed to find the foods that perform like this in your dog? Well, like everything: It takes a little bit of economics (buy what’s in your budget), a little bit of science (keep track of what you are feeding and observe and record the results) – and more than a little luck.
Does this sound daunting? C’mon, you can do this. You’re already doing it – you’re currently feeding your dog something, right?
The nutritional adequacy statement is also known as the “AAFCO Statement” AAFCO (The Association of American Feed Control Officials) is the nongovernmental group that develops and changes the model regulations for pet food that are adopted by the states. This statement tells the consumer which set of nutritional standards the product has been formulated to meet.
1. Check the “nutritional adequacy statement.” Some foods are not complete and balanced! If they are not, they must indicate that they are “for intermittent or supplemental use only.” These products are fine for short-term use, but they will not provide everything your dog needs over time.
Growing puppies have higher requirements for a number of nutrients than adult dogs. Complete and balanced dog foods must state whether they have been formulated to meet the nutritional standards for “growth” (puppies) or “adult maintenance.” If the label says the food is for “all life stages,” it has met the “growth” standards.
If you are feeding a dog who is still growing, you must check to see if the nutritional adequacy statement indicates the food is meant for dogs who are expected to mature to more than 70 pounds or less. For more information about these statements and feeding puppies, see “Puppy Needs New Food,” WDJ September 2020.
2 Note the amount of protein and fat in the food. You should have an idea of how much protein and fat you are already feeding your dog and whether that’s too much (is he overweight?), too little (is he underweight?), or about right. Look for products with protein and fat levels that are appropriate for your dog.
Be aware that these values range very widely in pet food; one can of food might contain three times as much protein or fat as another. Check the “guaranteed analysis” on the label of the food you have at home, and check it on any food you are considering.
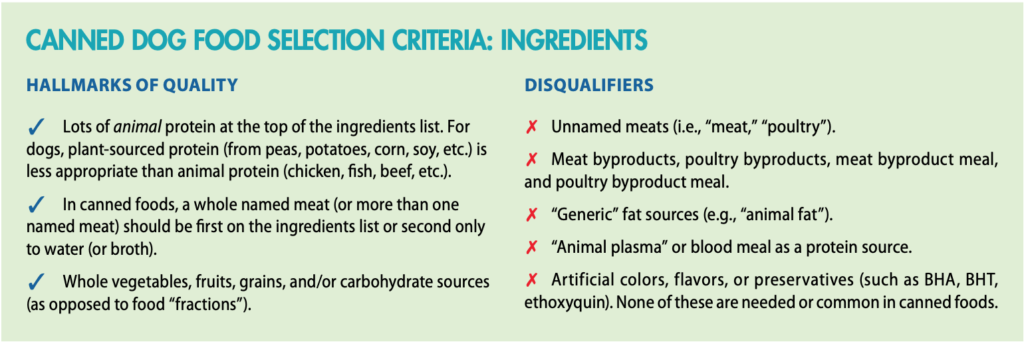
3. Now look at the ingredient list for hallmarks of quality. Look for things you can readily identify as food – real food. Chicken is chicken, but do you know what poultry by-product meal is? No? Then don’t buy it for your dog. (This sounds simplistic, but it’s a good guide when it comes to sorting out the higher-quality ingredients from the highly processed and not scrupulously managed waste products from the human food industry.)
For more guidance on what ingredients are acceptable and appropriate, see “Dog Food Selection Criteria: Ingredients” below.
4. Look at the ingredient list for what suits your dog – and what disagrees with him. If your dog is allergic to beef, don’t trust that a food manufacturer hasn’t changed its formula and added beef to that stew; check the ingredients every time you buy a food.
If you have observed that grains exacerbate your dog’s gas production, look for grain-free – or perhaps even carbohydrate-free foods. (Many grain-free foods are chock-full of alternative carbohydrate sources, such as peas, lentils, chickpeas, and other legumes; pumpkin; sweet potatoes, potatoes, and various byproducts of these ingredients (i.e., pea flour, pumpkin powder, etc.).
5. Any time your dog displays a change in his health, energy, appetite, or elimination habits, write it down somewhere. Note what you were feeding him. Keep track of when you change foods. Look for patterns in his response to various ingredients, protein or fat levels, or even different manufacturers’ products. Change accordingly!
COVID-19 Being Unfairly Blamed for Poor Customer Service
Reaching the pet food manufacturers with questions or concerns
right now is difficult – and that’s ridiculous.
Time to update the technology!
We’ve long advised readers to reach out to the makers of their dogs’ food if they have questions or concerns about the products – and to decline to buy food from companies who are not attentive to consumers or who can’t seem to provide basic information about the company’s products, such as a complete nutritional profile for any of its foods.
That advice stands today, even with the pandemic going on. Many people are working from home today; there is a wealth of technology available that should enable any customer service team to continue to communicate with consumers. But in the course of compiling information about the products featured on our “Approved Canned Foods” list, we had to call quite a few companies for information – and we heard an unprecedented number of recordings that stated no one was available to take our calls.
We understand that having someone available to provide knowledgeable support to consumers can be costly and difficult at times. But given the fact that our dogs’ lives depend on these foods, it seems like the least a pet food company can do is to equip some employee or the owner of the company with a cell phone so they can respond to consumer inquiries.
If you can’t reach anyone at a pet food company to ask a question about their products, our advice would be to avoid buying that company’s food. Period.
Mind Your Peas and Legumes
No correlation between DCM and these ingredients has been proven.
We’d advise limiting how much you feed to your dog anyway.
In recent years, there have been a plethora of headlines about a possible connection between certain canine diets and a potentially fatal health condition called dilated cardiomyopathy (DCM). Early reports blamed grain-free diets for causing DCM in dogs of breeds that were not usually predisposed to the disease. As more data were collected, the blame started to shift toward foods with a preponderance of peas, lentils, and other legumes.
In the past decade, these ingredients have become increasingly common in all dog foods, but especially so in grain-free foods, where they are used as both a carbohydrate substitute for grain and as a low-cost source of additional protein for the diet.
In reports that were part warning to pet owners, part fishing for news of previously unknown cases, the U.S. Food and Drug Administration (FDA) has published a series of announcements on the topic.
We published our own analysis of the FDA reports in “Diet, Dogs, and DCM,” in the November 2019 issue. We agree that there is reason to be concerned about feeding dogs diets that contain significant amounts of peas and/or lentils. As the article stated, “The FDA reported that 93% of all products involved in the reports they were investigating contained peas and/or lentils. Our analysis confirmed that 89% of the reported foods appeared to contain significant amounts of these ingredients (generally appearing before the first fat or in multiple combinations, sometimes with other legumes).”
Peas are a relatively new ingredient whose popularity has exploded in the last 10 years. The fact that so many foods today contain significant amounts of peas (and other legumes) and the increase in the number of dogs that are reportedly developing DCM (especially those in categories not typically associated with this disease) seems significant. Remember, however, that correlation does not equal causation; again, we are speculating, as
no one knows the cause at this time.
We recommend avoiding diets with legumes listed high in the ingredient list (before the first fat or oil) or that include several legumes, even if they appear lower in the ingredient list. Alternatively, it’s advisable to feed such diets on a short-term basis only, or as one of a number of legume-free foods in a rotation. In the table of “Approved Canned Foods”, we’ve noted which manufacturers offer products that have peas and other legumes appearing in moderate concentrations.
For more information about canine DCM and possible links to diet, please see the November 2019 issue.
APPROVED FOODS
Below, you’ll find a list of pet food companies that make the kind of foods that meet our selection criteria. You should notice that even among these better- and best-quality products, there is quite a wide price range. All of the products made by these companies are better than most of the products on the market. But some companies take food production to an art form, with certified humanely raised meats, organic ingredients, functional ingredients such as glucosamine, prebiotics, and probiotics, etc. Some of these products – more all the time! – are actually made in human food manufacturing facilities, which means they contain only human-edible ingredients. Wow!
But what’s most important is that you find products at the price point that you can afford and that suit your dog. So, to that end, we’ve included the price range of each manufacturer’s offerings, expressed by “price per ounce” (since can/carton/tub sizes are all different).
Using the steps described above, choose some foods that are new to you and your dog and give them a try! If your local pet supply store doesn’t carry them, try online. If the products really work for your dog, ask your local store manager if she can carry them for you.
And don’t forget: One-size-fits-all recommendations don’t work when it comes to diet. You have to feed the individual what works for him. It’s wonderful when you have more than one dog and they can both digest and thrive on the same variety of food, but we wouldn’t take it for granted that any two dogs can.
Whole Dog Journal’s Approved Canned Dog Foods for 2020
Products appear alphabetically by best-known name. In some cases this is the name of the company that makes the food; in others, it’s the name of the food line.
PRODUCT NAME/COMPANY INFORMATION
# OF VARIETIES
RANGE OF PROTEIN (as fed)
RANGE OF FAT (as fed)
PRICE PER OUNCE
NOTES
ARTEMIS OSOPURE
La Habra, CA
(800) 282-5876
artemiscompany.com
5
8%
4% - 6%
$0.28 - $0.34
All five varieties grain-free, and formulated for dogs in all life stages. Pea protein used in all varieties, @ 7th-8th on ingredients list.
AVODERM
(Breeder’s Choice, a division of Central Garden & Pet)
Walnut Creek, CA
(866) 500-6286
avodermnatural.com
13
5% - 9%
3% - 8.5%
$0.19 - $0.27
About half of the offerings are grain-free. All but two (weight control, vegetarian) are for all life stages. Peas appear @ 4th-8th on ingredients list.
AZMIRA
Tucson, AZ
(520) 886-8548
azmira.com
2
10%
5%
0.19
Both products formulated for dogs of all life stages. Lamb formula contains peas (7th on ingredients list). Whole brown rice used as carb source/thickener: Nice.
BIXBI RAWBBLE
Boulder, CO
(303) 666-1070
bixbipet.com
4
8.5% - 9%
8.5%
$0.28 - $0.34
All Rawbble canned foods are formulated for all life stages, and contain no grain, potato, tapioca, meals, or gums. (Pumpkin used as a carb/thickener, 4th-5th.)
All varieties are formulated for all life stages and are grain-free. Each contains pumpkin (@ 4th), peas (@ 5th-6th), and green-lipped mussels (@13th).
BUCKLEY LIBERTY
Boulder, CO
(720) 726-3193
buckleypet.com
3
8.5% - 9%
7.5% - 8.5%
0.26
Each variety is formulated for all life stages and is free of grain, corn, and soy. Each contains a single animal protein source but also peas (@ 3rd!). Sweet potato is used as carb/thickener (@5th-9th).
CLOUDSTAR WELLMADE
St. Louis, MO
(800) 361-9079
cloudstar.com
5
7%
3% - 4%
0.24
Each variety is formulated for all life stages and is free of grain, corn, soy, and potato. Pea protein appears in each (@4th). Sweet potato, pumpkin, tapioca starch, and/or chickpeas used as carb/thickeners (@ 5th-7th). Company says “made in a human grade facility.”
CORE (See WELLNESS)
DAVE’S PET FOOD
Agawam, MA
(888) 763-2738
davespetfood.com
29
7% - 10%
4% - 9%
$0.14 - $0.20
Dave’s offers five lines: 95% meats, grain-free, “naturally healthy” (with rice), “restricted diet” (each addresses a medical issue and most are not complete & balanced), and “stewlicious.” Not thrilled with company’s incomplete AAFCO “nutritional adequacy” statements on website.
EAGLE PACK
(Wellpet) Tewksbury, MA
(800) 225-0904
eaglepack.com
4
9%
6%
$0.17 - $0.18
All varieties are formulated for dogs of all life stages. Each food contains brown rice (@ 4th) and some also contain barley (@ 5th). No peas or other legumes.
FIRSTMATE, KASIKS
North Vancouver, Canada
(800) 658-1166
firstmate.com
14
8% - 12%
3% - 8%
$0.27 - $0.40
Made in Canada. Company says chicken and turkey used in all varieties are cage-free, salmon and tuna are wild-caught. Many varieties are grain-free and extremely low-carb. Many varieties use a single animal protein source. All varieties are formulated for dogs of all life stages. Firstmate owns and operates its own cannery.
FROMM
Mequon, WI
(800) 325-6331
frommfamily.com
32
7% - 10%
2% - 8.5%
$0.20 - $0.39
Fromm offers three lines: Shredded meats, vegetables, and legumes in gravy; pâtés contain meat, legumes, potatoes, and vegetables; “Frommbalya” stews contain potatoes, rice, and peas. All varieties are formulated for dogs of all life stages. Fromm owns and operates its own cannery.
GO!
(Petcurean) Chilliwack, British Columbia
(866) 864-6112
petcurean.com
14
7.5% - 10%
2.5% - 8%
$0.30 - $0.32
All varieties are formulated for dogs of all life stages. Some varieties are packaged in Tetra Pak cartons. Some varieties contain grain and other carbs, others are grain-free. Always read the ingredients list: A few varieties include porcine plasma (we’re not fans of this ingredient).
HALO
Tampa, FL
(800) 426-4256
halopets.com
9
5.75% - 11%
3.5% - 9%
$0.32 - $0.44
All varieties formulated for adult maintenance except one: the “Puppy” variety. Peas, pea flour, and/or pea fiber appear in many varieties. Three varieties are grain-free.
HEALTH EXTENSION
Melville, NY
(800) 992-9738
healthextension.com
15
7% - 9.5%
2% - 9%
$0.20-$0.21
All varieties formulated for adult maintenance only. Most varieties are grain-free; three are 95% meat. Company offers a few novel protein varieties (quail, rabbit, venison).
HOLISTIC SELECT
(Wellpet) Tewksbury, MA
(800) 225-0904
holisticselect.com
6
11% - 12%
6% - 7%
$0.25 - $0.28
All varieties are formulated for all life stages, all are grain-free pâtés. Ground dried peas appear (@ 4th-6th) in each formula, as does potato protein (@ 5th-8th).
HOUND & GATOS
(Gott Pet Products) St. Francis, WI
(888) 896-2951
houndgatos.com
11
10% - 13%
3.5% - 10%
$0.29 - $0.60
All varieties are grain-free, 98% meat. Are products formulated for all life stages or adult maintenance? Website doesn’t say; label suggests ALS but isn’t explicit. In our opinion, this is irresponsible.
INSTINCT
(Nature’s Variety) St. Louis, MO
(888) 519-7387
instinctpetfood.com
13
8.5% - 11.5%
3% - 8.5%
$0.23 - $0.60
All except the three “limited ingredient” varieties are formulated for all life stages. No grain, potatoes, corn, wheat, or soy. Peas appear @6th-9th on ingredients of most varieties, higher (@4th-5th) in limited-ingredient varieties.
JUST FOOD FOR DOGS
Irvine, CA
(866) 726-9509
justfoodfordogs.com
4
6% - 10%
4% - 7%
$0.40 - $0.48
Foods packaged in Tetra Paks; company says foods are made in a USDA kitchen with 100% human-grade ingredients. All varieties except Chicken & Rice are formulated for adult maintenance only. One (Beef & Potato) contains peas.
KASIKS (See FIRSTMATE)
KIWI KITCHENS
Christchurch, New Zealand
(64) 21 706621
kiwikitchens.nz
11
7% - 10.7%
1% - 7.5%
$0.30 - $0.42
All varieties formulated for dogs of all life stages. All contain 93% meat from a single animal protein source. Two varieties are made with green tripe (lamb tripe, venison tripe). Made in New Zealand.
KOHA
Delray Beach, FL
(800) 478-7713
kohapet.com
20
8% - 12%
2% - 11%
$0.24 - $0.54
Koha offers two lines: limited or minimal ingredients, and “homestyle stews.” All “limited ingredient” varieties save one (Venison) are formulated for adult maintenance only. Each contains 90% meat from a single animal protein source. All but one of the stews (Beef & Salmon) are formulated for all life stages. Koha is made in three locations (U.S., Canada, Thailand).
LOTUS
Torrance, CA
(888) 995-6887
lotuspetfoods.com
16
8% - 14%
4% - 10%
$0.29 - $0.48
All varieties are grain-free and formulated for all life stages. There are three types: loafs, stews, and “just juicy” (95% meat) varieties. Loaf varieties use pea flour (@3rd-5th) and sweet potatoes as carb source. Stews contain no peas or other legumes. Lotus owns and operates its own cannery.
Fifty-seven varieties? Oy. Some are sold only seasonally. All are grain-free. Some are for adult maintenance, some are for all life stages; some contain peas; some are legume-free; some are 96% meat or limited ingredient varieties. Always read the ingredients list!
NATURAL BALANCE
(J.M. Smucker) Burbank, CA
(800) 829-4493
naturalbalanceinc.com
18
5% - 9.5%
3% - 8%
$0.19 - $0.23
Only about half of these are formulated for all life stages; check the label. Most do not contain legumes, instead using rice, potatoes, and/or sweet potatoes as carbs; some also contain meat and meat meal (unusual for canned foods).
NEWMAN’S OWN
Westport, CT
(203) 222-0136
newmansown.com
8
8% - 10%
5% - 12.5%
$0.19 - $0.24
Half of the company’s offerings are 95% organic; the rest are made with a preponderance of organic ingredients: Nice! All are formulated for adult maintenance only.
NULO
Austin, TX
(512) 476-6856
nulo.com
30
7% - 10.5%
3% - 12%
$0.21 - $0.39
Most of these foods are formulated for adult maintenance only; all are grain-free. Company says the varieties packed in cartons (Tetra Paks) are made in a human food facility (all “human grade” ingredients). Products in conventional cans all contain legumes and/or sweet potatoes.
NUTRISOURCE, PUREVITA
(KLN Family Brands) Perham, MN
(800) 525-9155
nutrisourcepetfoods.com
20
8% -12%
4.5% - 9%
$0.14 - $0.24
All varieties are formulated for all life stages. About half of the Nutrisource varieties are grain-free and contain legumes (the grain-inclusive ones use rice or barley). PureVita formulas are all grain-free and 96% meat.
OPEN FARM
Toronto, Ontario
(833) 399-3403
openfarmpet.com
4
8%
5% - 6%
0.64
Company says all meat sources used are certified humane and 100% of the ingredients are “human grade.” Products packaged in Tetra Paks. All varieties except one (Harvest Chicken Rustic Stew) are formulated for all life stages.
PARTY ANIMAL
West Hollywood, CA
(855) 727-8926
partyanimalpetfood.com
8
9% - 11%
5% - 12%
$0.29 - $0.31
All varieties are grain-free, limited-ingredient, and formulated for adult maintenance only. Cocolicious line uses one animal protein source and coconut.
PETGUARD
Sewickley, PA
(929)-515-1436
petguard.com
8
7.5% - 9.5%
4.5% - 8%
$0.24 - $0.30
All varieties but two (Turkey/Sweet Potato, Chicken/Brown Rice) are formulated for adult maintenance only. Two varieties (Chicken/Vegetable and Vegan) are organic.
PET-TAO
Franklin, TN
(615) 934-3832
pettao.com
2
8%
6%
0.32
PetTao’s foods are formulated for all life stages, according to the principles of Traditional Chinese Veterinary Medicine’s food therapy.
PUREVITA (See NUTRISOURCE)
RAWZ
York, ME
(844) 480-8672
rawznaturalpetfood.com
14
9% - 11%
1% - 9%
$0.27 - $0.37
96% meat formulas are formulated for all life stages; shredded meat and “hunks” varieties are for adult maintenance only. None of the products contain grain or gums, using tapioca starch and pumpkin for a carb source/thickener.
REDBARN
Long Beach, CA
(800) 775-3849
redbarn.com
13
8% - 15%
4% - 9%
$0.20 - $0.25
All varieties are grain-free and formulated for all life stages. Most of the pâté varieties contain peas (@ 4th-5th). All but one of the stew varieties (Beef) contain peas (@4th-9th).
SIMPLE (See WELLNESS)
SOLID GOLD
Chesterfield, MO
(800) 364-4863
solidgoldpet.com
14
7.5% - 9.5%
3% - 8.5%
$0.20 - $0.69
Five of the 14 varieties are formulated for adult maintenance only (Fit & Fabulous, Green Cow, Leaping Waters, Sunday Sunrise, Hund-N-Flocken). Twelve varieties are grain-free. Mighty Mini varieties are packed in tubs, not cans.
STELLA & CHEWY'S
Oak Creek, WI
(888) 477-8977
stellaandchewys.com
6
9% -10%
2% - 3%
0.36
All six varieties are formulated for adult maintenance only. Beef, chicken, lamb, turkey varieties use a single animal protein source; two “medley” varieties mix animal protein sources. Packaged in Tetra Pak cartons. All are free of grains, legumes, and gums – and company says the products are 100% human-grade. Sold only in independent “neighborhood pet supply stores,” not online or in chain pet supply stores.
TASTE OF THE WILD
(Diamond Pet Products) Meta, MO
(800) 342-4808
tasteofthewildpetfood.com
5
7.5% - 9%
3.5% - 4.5%
0.17
All varieties are formulated for all life stages. Each contains peas (@7th-9th), potatoes, and/or potato starch. Creative “ingredient splitting” with the water sources in the ingredients lists (to avoid having water appear first): For example, in the Southwest Canyon variety, ingredients are “beef, beef broth, lamb broth, vegetable broth, beef liver...” Aw, c’mon!
THE HONEST KITCHEN
San Diego, CA
(866) 437-9729
thehonestkitchen.com
6
8% - 12.5%
2% - 8%
0.33
All varieties are grain-free and formulated for all life stages. Peas appear in just one variety (Salmon/Chicken Stew). Products are packaged in Tetra Pak cartons. Company says products are 100% human edible and made in a human food facility. Company includes a full nutrient analysis of each product on its website; we’re in love.
TIKI DOG
Chesterfield, MO
(866) 821-8562
tikipets.com
27
7% - 17.1%
2% - 12%
$0.24 - $0.66
Some TikiDog foods are formulated for all life stages; others are for adult maintenance. Some are packaged in large cans, some in small cans, some in plastic tubs. Some are manufactured in Thailand, some in the U.S. Read the labels!
ULTRA
(Nutro, a div. of Mars) Franklin, TN
(800) 833-5330
nutro.com
14
8% - 9%
3% - 7%
$0.51 - $0.57
We prefer the Ultra line over the rest of the Nutro foods. All of these foods are formulated for adult maintenance only and seem to be offered only in small tubs now. Porcine plasma shows up in a few varieties; read the ingredient list!
All varieties are formulated for all life stages; all are free of carrageenan. Five varieties are grain-free, seven contain grain. About half contain peas (@5th - 7th).
WALK ABOUT
New Holland, PA
717-519-7622
walkaboutpetproducts.com
5
7.5% - 8%
2%
$0.15 - $0.33
All varieties are grain-free, contain peas (@5th), are formulated for adult maintenance, and contain a single novel animal protein source (boar, duck, kangaroo, rabbit, quail), and contain peas (@5th). We advise saving these for dogs with proven allergies to common proteins.
We like this company, but as with Merrick’s foods, we don’t get the need for so many varieties: pâtés, stews, cans, plastic tubs, limited ingredient, grain, grain-free, 95% meat: You name it, they make it. About half are formulated for adult maintenance only, so check the label. Note that “growth and maintenance” is the same thing as all life stages.
WELLMADE (See CLOUDSTAR)
WERUVA
Natick, MA
(800) 776-5262
weruva.com
20
6% - 10%
1.2% - 6%
$0.29 - $0.35
All products are formulated for adult maintenance and free of grain and carrageenan. Peas, potato starch, pumpkin, and sweet potato are used in various combinations as carb sources/thickeners. Products are manufactured in Thailand in a human food facility.
WET NOSES
Monroe, WA
(866) 938-6673
wet-noses.com
8
10% - 14%
4.5% - 7%
1
Gorgeous, crazy expensive food packed in glass jars. Website fails to state this, but all foods are formulated for adult maintenance. No legumes included; some varieties contain rice or barley, others are just meat and veggies.
All foods are formulated for dogs in all life stages. All varieties are grain-free, start their ingredient lists with a whole, named meat, and all contain peas (@4th - 6th).
ZIGNATURE
(Pets Global) Valencia, CA
(888) 897-7207
zignature.com
13
8% - 11.5%
4% - 7%
$0.25 - $0.32
All foods are formulated for all life stages; all but one contain a single animal protein source (the outlier is Zssential, which uses several animal proteins). None contain grain; all contain legumes including peas (@3rd - 7th) and chickpeas. Many varieties use novel protein sources (catfish, duck, goat, guinea fowl, kangaroo); we advise saving these for dogs with proven allergies to common proteins.
Adopting siblings can work, but it takes a truly special owner who has double the time and energy to give to puppyhood. These sisters, Icebox and Spaz, have committed owners who knew how much extra time it would take to make a littermate adoption succeed.
I hear it all the time: “Honey, maybe we should get two! Look how much they love each other! How can we possibly split them up?”
My family and I frequently foster litters of rescue puppies, and when approved adopters come over to make that big decision – which one will it be? – the conversation often takes this detour. Watching two darling pups snuggling or romping together, somebody says, “Why don’t we just take two?”
It’s a natural impulse. In fact, keeping littermates together was very much my own hope when we fostered our first litter almost a decade ago. Back then, when a potential adopter epressed an interest in getting two pups, my heart raced. Think of it: Little Ben and Pretty Girl, together forever! I loved this idea! The advantages quickly added up in my mind:
* The transition would be so easy! No sad pup crying through those initial nights without the warmth and company of littermates.
* The pups would be so happy to have a friend to play with every day.
* There would be guaranteed exuberant exercise, which would decrease household destruction and mouthiness.
* The owners would be less stressed by the demands of puppyhood because, rather than having a bored puppy constantly seeking their attention, they’d have two pups pretty darned content with each other. After all, I vastly preferred fostering two pups to one, because it was way less work for me.
Filled with excitement, I let the shelter know that one of our potential adopters wanted two puppies. Their response? “We don’t actually adopt out littermates together.” I was stunned. What kind of anti-puppy-happiness policy was this?
A PREPONDERANCE OF CONS
It turns out I had a lot to learn. While every one of the bullet points above is true, there are even more bullet-point reasons why most dog trainers and animal shelter professionals recommend against adopting littermates, including:
* Puppies need to learn to be alone. One of the key things I try to teach my foster pups is that they’re okay without their littermates. If I were to let them hang out in the same room with their mom and siblings every single minute for eight weeks, then adoption day would be terrifying for them. In the beginning that means simply holding one pup outside of the puppy pen for a moment, and immediately returning. Then I might take just two pups into the kitchen to play while I do the dishes. Finally, I’ll take just one pup upstairs with me to hang out with a chew toy while I work on the computer.
Adopting siblings can delay this vital bit of the puppies’ education indefinitely. Now there are two pups who may have never taken one breath when they weren’t next to another pup. The longer that goes on, the more deeply attached they become. Some owners realize they have a giant problem only months later when they casually separate the pups – perhaps for a vet appointment – and find both dogs in an absolute panic, destroying walls and escaping from crates.
Littermates Twilight and her brother TikTok joined a family that includes anther dog and three cats, so the duo is rarely alone together, and each gets critical one-on-one time with their human.
Of course, you can combat this issue just the way I do with a litter at my house: by making time to take each pup alone somewhere, every day. They need to have regular, varied experiences where they are separated from their siblings: in the house, on a walk, in the car, on a playdate. If you have the time and perhaps the household structure to allow that, this may not be a problem. However, experienced trainers and shelter staff will tell you thatmost owners find they barely have time for one pup, much less two – even though they thought they were prepared.
* Having an always-present playmate isn’t enough to properly socialize a puppy. Daily play with a live-in packmate helps tire out both puppies, which is great – but the giant downside is that, without the urgent impetus to find another puppy or dog to help tire out a singleton pup, owners tend to get complacent.
A lone puppy’s chewing, biting, and jumping will push a good owner to seek out other dogs to exhaust the little guy, which enlarges the pup’s world beautifully. There is far greater value in playing with all kinds of dogs – big and small, runners and wrestlers, floppy-eared and pointy-eared. They each play differently, and by interacting with a number of play partners, a pup learns a more nuanced, expanded language of doggy communication. That, in turn, makes the puppy comfortable with future dog encounters – on leash walks, at your sister’s house for Thanksgiving, at the beach with your friend’s dogs.
In contrast, the littermates who play only with each other may well end up being dogs who can play only with each other! Unaccustomed to play styles they are unfamiliar with, less-socialized dogs may take offense at playful overtures from dogs who are new to them, and erupt in defensive aggression out of fear.
Again, an owner who is well aware of this issue can completely mitigate the effects by arranging for plenty of play time with other puppies and dogs as the puppy matures.
* When people own two puppies, they tend to take the pups on fewer walks and adventures. When I first started fostering, I was always drawn to the adopter whose application mentioned their big fenced yard. Sure, the city apartment dwellers said all the right things, but then I’d think about this little pup who’d have to go down an elevator and then pass strangers and hear loud trucks every time he just had to pee! “Poor pup,” I thought.
I’d like to slap my old self. I’ve learned over the years that those city dogs become fabulously socialized! Because exposure to all of those things is an automatic part of their life, they inevitably become incredibly relaxed about it all. It’s wonderful.
What does that have to do with littermate adoptions? Well, often littermates don’t get out into the world if they live in the same house. They are nicely tired from all of their playing, so they don’t nudge their owners into walks. And even if they do, sometimes the owner remembers that last walk where two dogs were awfully hard to manage and opts out.
Again, the dedicated owner will get around this by remembering how critical it is to get a young pup out and about in the world and will make the time (and enlist the helpers) to make adventures into the wider world a regular part of the routine for both puppies – preferably, one at a time, for most of those walks.
* It’s more than twice as hard to train two puppies than it is to train one. I love to teach young pups to sit, stay, spin, touch, and shake. In fact, I really can’t help myself – whenever I have just one pup here. But if I have more than one pup? The best I can do is “sit.” I’m a dog trainer, for goodness sake, and I can’t teach two dogs a new thing at the same time.
Teaching well requires giving split-second feedback to the dog. When you have two dogs doing different things, the feedback loop becomes meaningless. “YES!” you say as Pretty Girl sits nicely. But Little Ben heard that too, while he was jumping up on you. Hmm. What exactly did he just learn?
To train two pups, you need to separate them. And perhaps the trainee needs to be out of earshot so that the distressed barking of the left-out pup does not distract our student of the moment. Do you have a set-up where you can easily take one pup away and work with her a few times a day – and then turn around and do that with the other pup? Can you sustain that for a year? Maybe you can!
But most can’t, and, sadly, what often happens is that an owner calls a trainer in tears, reporting two completely unruly 9-month-old dogs who “can’t” be walked. The pups are bonded strongly to each other, but not with the owner. It’s a heartbreak that often results in one, if not both, being rehomed.
THE IDEAL SCENARIO
Lots of individual training plus the owner’s robust support system has made the adoption of brothers Bristol and Bedford work beautifully. They are each other’s best friend and comfort – but they also settle down just fine when separated.
Trainers and shelter staff will almost always advise against a littermate adoption; instead, they frequently give the very sound advice to simply wait a year, so that your well-trained adult dog can set a fantastic example for a new pup.
That said, taking in two siblings might be the right decision for you. The key is to be fully informed about the tricky issues and committed to a plan. When that happens, it can work out beautifully.
As I was preparing to write this article, I reached out to a handful of people who adopted littermates from my rescue group. Every one of them wrote back using exclamation points about how much they love their doggies and how the double adoption was the perfect approach for them. My follow-up questions revealed that these folks truly walked the walk. They’ve poured a lot of time and resources into these pups, carefully shaping their experience so that each dog is well trained and confident on their own – and also darling together. Clearly, it can be done.
Even so, any time I hear an adopter say, “Hey honey, how about two?” I’ll still suggest my very favorite option: “Do you have a neighbor who needs a puppy?” That’s the best of all worlds: each of the pups will have a buddy close enough so they can get happily tired from everyday playdates, the owners can get little breaks while their pup is visiting next door, and each puppy will get plenty of individual attention back at home.
A dog who is going to live with children shouldn't merely tolerate kids; she should adore children - and even prefer playing with them to being with adults. This dog is friendly, but not all that interested in the little girl
Those of us who love dogs find the prospect of bringing home a new canine family member intoxicating and exhilarating. Well-planned in advance or not, the adoption of a new dog likely triggers a rush of oxytocin unparalleled by all but a few other high-end life experiences.
That said, while some spur-of-the-moment adoptions can and do turn into successful relationships, when possible, we highly recommend that your next dog adoption be well thought out in advance, and you select your new dog carefully, to maximize the likelihood that you will be able to provide a lifelong loving home for the fortunate canine who joins your family.
THINK IT THROUGH
The process of adopting a dog can be daunting. We encourage you to do some pre-planning before you start looking for the newest member of your family, to increase the chances that you will find an ideal lifetime companion.
If you are single and living alone, you are free to consider only your own needs and wants; the process becomes considerably more complex if you have family or housemates. In either case, before you begin your search in earnest, it behooves you to think about your prerequisites and preferences, including:
• Family/roommate buy-in. Is everyone in the household on board with getting a dog (or another dog)? If not, work through all the reservations before you proceed any further. It doesn’t benefit the dog to bring her into a home where there will be simmering resentment or outright conflict over her presence.
• Breed and source. Do you already have your mind set on a specific breed or breed-type? If so, does everyone in the family or household feel comfortable with your choice? Have you researched the breed thoroughly so you understand its behavior propensities and common medical issues?
If you are looking for a particular breed or type, you might consider adopting from a breed rescue group, getting pre-approved and putting yourself on a waiting list at your local shelters, or purchasing from a reputable breeder. Private-party adoptions are also a reasonable option – a friend or co-worker who needs to rehome a canine companion, or even, carefully, a private adoption from a classified ad, or Craigslist. No pet-store puppies, ever, please. (For more about where to look for your next dog, see “Adopt or Shop,” WDJ August 2020.)
• Size. If you don’t already have a breed in mind, does size matter? If so, what size dog are you considering – toy, small, medium, large, or giant?
Be aware that toy and giant breeds are at greater risk for significant medical problems. In general, the giant breeds tend to have short life spans while the smaller breeds tend to live longer. A recent analysis of veterinary records revealed that dogs under 20 pounds had an average lifespan of 11 years, with some smaller dogs living as long as 14 years or more, while those over 90 pounds typically lived for an average of only eight years. Small dogs may be a greater tripping risk – but they are more portable! – while large and giant breeds may be more likely to knock you over (or your senior grandparent).
• Age. Puppies are undeniably adorable. On the plus side, starting with a baby dog means you can have a huge influence on her development and know that her world has been force-free from very early on. Still, that’s not a guarantee that she will turn out to be the perfect dog, especially if she wasn’t well socialized before you adopted her. (Despite what you may have heard, an eight-week-old puppy is not a “blank slate.”) And they are a lot of work.
As we recently contemplated the adoption of a 3-month-old Australian Cattle Dog-mix, my husband and I realized that we don’t want to adopt a puppy. They are a lot of work!
In contrast, adult dogs are more likely to be a “what you see is what you get” proposition – although they can deliver behavioral surprises too, as they adjust to their new life with you. They are past the “needle-sharp puppy teeth” stage, thus less likely to shred your flesh (and your possessions) with puppy mouthing. And while some adults still may enjoy chewing, there’s a good chance they will be less destructive (barring anxiety-related behaviors) and are more likely to already be house-trained (or easily house-trained).
On the other hand, it’s also possible that they may come to you with some already-well-established behavior challenges…
• Coat. Are you thinking short or long coat? Does it matter to you? It matters a lot to some people.
First, consider grooming. Is someone going to be happily responsible for brushing that long Afghan Hound, Collie, or Pomeranian fur on a regular basis – at least once a week, and maybe more? Will you happily bear the cost of routine trips to the groomer for that Poodle or Doodle clip? Will your Roomba handle the carpet of long white Great Pyrenees fur that covers your rug?
You’re not off the hook with short-coated dogs either – those prickly Labrador Retriever hairs are great at infiltrating the fabric of your furniture (or business suit) and can be a bear to get out! Of course, there’s always the Mexican hairless dog… the Xoloitzcuintli (pronounced “show-low-eats-QUEENT-lee”).
When considering an adoption prospect, those of us older adopters would be wise to consider our own health, strength and energy level, in addition to the dog’s. The fact that we have owned big dogs our entire lives is, sadly, not a guarantee that we can still safely handle one for the next 10 or so years.
• Dog-keeping details. Which family members will be responsible for which dog-related chores: feeding, clean-up, walks, grooming, trips to the vet, training? Where will the dog sleep? Is she allowed on the furniture? Who will be your vet, groomer, pet sitter, dog walker? There is an endless array of minutiae that comes with sharing your life with a dog; the more of the details you work out in advance, the better!
SELECTING YOUR DOG
Okay: You’ve given all of the previous prerequisites and preferences some consideration. You’ve read the “Adopt or Shop” article in the August issue of WDJ, so you know where you are going to look for your next dog. It’s time to go meet some prospects!
When my husband and I both worked at animal shelters, selecting our next dog was easy. We never actually set out to look for one; instead, while we met dozens of dogs every week, sooner or later a dog would enter the shelter that one or the other of us would have a near-instant connection to. Our “love at first sight” moments would then be enhanced by the opportunity to get to know the dog better over the next few days as he went through the intake process.
Since leaving shelter work, we’ve learned just how challenging it can be for most people to find the perfect dog! You go to the shelter or rescue meet-and-greet location, you see a dog that appeals to you, spend a few minutes with him, and the next thing you know you’re filling out adoption papers. You wouldn’t get married that way!
Today, it’s common for people to receive very little information about the dog they adopt. When we worked in shelters, we would get extensive information from owners who were surrendering their dogs. We generally had less information about stray dogs that our officers picked up, but at least we conducted behavior assessments (flawed as they may be) and kept notes on the dog’s behavior during her stay with us. Anything we learned about the dogs was passed on to the adopter.
In contrast, today it seems like few organizations have much information about their dogs other than “she came from a shelter in North Carolina.” They sometimes don’t even seem to know if the dog was owned or stray! When it’s time to adopt, you may have to rely entirely on your own observations and instincts about the dogs you meet – and purchasing from a breeder can be equally fraught with challenges.
Here are some suggestions to help you succeed in your adoption quest:
* Get help. If your adoption organization doesn’t provide skilled adoption counseling and you aren’t confident in your own abilities to make a good choice, consider taking a dog-savvy friend with you, or even paying a qualified force-free professional to help you with your search. The same holds true if you are purchasing from a breeder. Take someone with you, unless you are 100% confident that the breeder is ethical, knowledgeable, and well-qualified to you help you select your pup.
* Insist on meeting the dog in person. I am a professional dog trainer/behavior consultant and I wouldn’t even consider adopting a dog sight unseen. I don’t care what information or assurances the organization has given you, or how many videos of the dog you have watched – you don’t know who the dog is until you meet him.
I am appalled by the prevalence of internet adoptions happening these days with no actual meeting between dog and human until after the paperwork is signed and sealed and the dog is delivered halfway across the country. While it is fairly common practice for breeders to ship puppies across the country (or across oceans!) to buyers, sight unseen, I wouldn’t do it, no matter how great the breeder’s reputation.
* Know what you’re looking for (as described above) – and also know which qualities might be negotiable. Perhaps you’re looking for a female Border Collie and you go to the shelter and the most perfect male Australian Shepherd is there in the kennel, begging you to adopt him. Close enough? Maybe so!
It doesn’t necessarily even have to be that close. A husband/wife couple, clients of mine, were recently looking to adopt a small dog. They went to the shelter to meet a 20-pound terrier-mix they had seen on the website, but when they got there the dog was already adopted. They came home with a purebred Akita who is one of the nicest dogs I’ve met in a long time. They are quite thrilled with their new family member.
Too scared to approach you? Do not adopt unless you want a “project” dog who may never get comfortable with humans.
* Resist the pity party pup. It’s easy to feel sorry for the poor, scared dog huddled in the back corner of her kennel run. But you should know that if you adopt this dog there’s a very good chance you are looking at a significant behavior-modification project; it’s possible that this dog will have fear-behavior challenges for the rest of her life. Note: I am a dog behavior professional and I would not adopt such a dog!
Truth be told, most people want a behaviorally healthy dog they can take with them to the beach, to the office, to their child’s soccer game, on hikes, to family reunions, to dog training classes – and shy, frightened dogs may never be able to do those things. Adopt only if you enjoy the challenge of a behavior modification project and understand the possible long-term ramifications of adopting a fearful dog.
* Consider foster-to-adopt. More shelters and rescue groups now offer this as an option, both to give you a chance to evaluate the dog in a home setting and to free up shelter and foster home space for incoming dogs. Fostering can give you and the dog the opportunity to see if it is a good fit – and allows you to feel less guilty about returning the dog if it doesn’t work out. You hadn’t made a full commitment, and you are now able to provide the adoption agency with information that can help them make a better fit with another adopter.
* Conduct your own behavior assessment. It doesn’t have to be as extensive as the ones that some organizations utilize, but there are some basic things you can do to see how the dog responds and make adoption decisions accordingly.
A DO-IT-YOURSELF BEHAVIOR ASSESSMENT
Studies in recent years have found shelter assessments to be unreliable and non-predictive; behaviors seen in assessments are often not seen in the adoptive home after the dog leaves the shelter, and behaviors not seen in the assessment may appear after the dog is in a home. Even so, it helps to walk through a structured assessment, if only to extend the amount of time you spend with the dog before making a commitment.
I’m not suggesting you do an extensive assessment protocol, just try a few reasonably non-aversive things to see how the dog responds. If you’re headed out to assess a potential new family member, take this list with you and circle the appropriate letters for the behaviors you see. Having a rubric like this can help guide you to a smart decision.
Before you start, ask if the shelter or rescue group is comfortable with you performing an assessment, and share with them the protocol you intend to use.
1. Watch the dog. Before actually interacting with the dog, observe her from a distance. Is she:
[A] Comfortable and relaxed in her kennel or other housing? (This would be ideal.)
[B] Pacing, stressed, and barking?
[C] Charging at dogs and humans who pass?
[D] Huddled in the back?
Note that B, C, and D are red flags; however, some dogs who are stressed or fearful in the kennel are reasonably normal when in a less intimidating environment, so this doesn’t have to be a complete rule-out.
It’s wonderful when you find a dog who walks super nicely on a leash. Not walking on a leash is not necessarily a deal-breaker, however.
2. Walking on leash. Out of the kennel and on leash, does she:
[A] Walk happily with her handler? (This is ideal.)
[B] Pull hard on the leash and/or sniff? (This is your basic training project.)
[C] Flail wildly or put on the brakes and refuse to move? (This represents a more significant training and/or behavior challenge.)
3. Take her off leash. In a safely enclosed area, remove her leash. Does she:
[A] Happily greet and stay somewhat near humans? (This is ideal affiliative behavior.)
[B] Cling desperately to humans? (This might be fear or separation-related behavior.)
[C] Confidently explore the room with occasional check-ins with the humans? (This is nice, somewhat independent behavior.)
[D] Confidently explore the room and ignore humans? (This might indicate a very independent dog, which can be challenging.)
[E] Go wild and crazy, racing around the room non-stop with glee? (High-energy dogs can be a challenge.)
[F] Pace back and forth, perhaps whining, never calming or settling down? (A stressed, anxious dog can be a significant behavior challenge – or could settle once out of the shelter environment.)
[G] Cautiously explore the room? (She may lack confidence and need some behavior modification.)
[H] Hide in a corner and refuse to move? (This is a very fearful dog who will need extensive behavior modification.)
This affectionate dog loves being handled and touched all over, but her contact is loose and relaxed. An anxious, insecure dog would be more clingy and tense.
4. How is she with handling? With the leash back on, do some general handling: Pet her all over, touch her paws, look in her ears, look at her teeth. (Stop at any time if she appears uncomfortable or resistant to a degree that is unsafe.) Does she:
[A] Enjoy your touch, warm and wiggling and asking for more? (Best.)
[B] Tolerate your touch but not really enjoy it or invite more interaction? (This is acceptable if you aren’t looking for a touchy-feely snuggle-dog.)
[C] Move away from you? (If she’s clearly not comfortable with handling, she may be a behavior-modification project.)
[D] Freeze, give you a hard stare, growl, and/or snap? (These indicate significant behavior issues; do not adopt unless you are a behavior professional or very skilled and experienced dog owner looking for a project.)
5. Check for any training. Ask the dog to sit, lie down, and shake – three behaviors that owners are most likely to have taught her. Then see if you can get her to do anything by luring with treats that you brought with you. Does she:
[A] Appear to have already have some training? (This is best.)
[B] Easily perform new behaviors that you try to get her to do with a treat? (This is also great.)
[C] Show interest in the treat but doesn’t understand what you are trying to get her to do? (This is acceptable; she may just need more time and patience to help her understand.)
[D] Show no interest in the treat? (She may be too stressed to be interested in food – but her lack of interest in food may present a more significant training challenge.)
6. Is she playful? Try offering the dog a variety of toys you have brought with you – a ball, a stuffed squeaky toy, a tug, a food-dispensing toy. Start with gentle play; you can intimidate some dogs if you play with them too much or too hard. Does she:
[A] Play with you happily and appropriately? (This is best.)
[B] Play with you happily but gets too aroused and a little mouthy? (This is acceptable, but she will need management and training.)
[C] Love to play with the toys but gets a little (or a lot) tense when you try to take the toy? (This indicates a tendency to guard her “stuff,” better known as resource-guarding; she will need management and training to improve this behavior.)
[D] Declines to play at all? Avoids you or looks at you like you’ve lost your mind? (This is okay if you don’t mind a dog who doesn’t play, or you want to try to teach her to play; see “Let the Games Begin,” November 2014.)
A dog who favors attention from and interaction with a child over an adult is an ideal prospect for a family with kids.
7. Kid considerations. If you have children you must have your potential dog meet them before finalizing the adoption. Some dogs who are perfectly wonderful with all of the above simply cannot live with children. For a dog to live safely with children she should adore them, not just tolerate them. When the dog sees your child or children, does she:
[A] Appear happy to approach and interact appropriately, as if she were saying, “Yay! Kids!”? (This is best.)
[B] Appear happy to approach and interact, but is a little too excited? (She will need management and training.)
[C] Appear to ignore or tolerate the presence of the child or children? (If you have kids, this is not acceptable; do not adopt this dog.)
[D] Is she cautious, fearful, reactive or aggressive? (Do. Not. Adopt!)
8. Do you have other dogs? Ideally, you will have brought along your home dog(s) so they can be introduced in a neutral environment. If not, if at this point you are still very interested in the dog, ask to have the dog put on hold so you can go home to get your home dog(s) for an introduction. Introduce them carefully, of course, and again, have a qualified dog training professional or dog-savvy friend present to help.
When the dogs see each other from across the room or yard, do they:
[A] Both appear reasonably calm and happy to approach and meet each other? (This is best.)
[B] One appears more assertive, the other more appeasing? (This is also great, as long as the more assertive dog doesn’t come on too strong.)
[C] Both appear happy to approach but are very excited? (This is acceptable, though you will need to manage their behavior with each other.)
[D] Dogs ignore/avoid each other? (This is not a good choice; avoidance often turns into a significant behavior challenge.)
[E] Either or both dogs show signs of tension: stiff body language, hard stares, growling, reactivity? (This is not a good choice.)
9. Do you have other animals in your family? If you have other small or large companion animals (cats, pigs, birds, horses, etc.), ask if the dog has any history around those, and if there are any available on the premises where you are meeting the dog. With the dog on leash at a distance, observe her behavior. Does she:
[A] Watch calmly from a distance? (This is best.)
[B] Watch with happy excitement from a distance? (This is okay, though she will need management and training.)
[C] Become highly aroused and /or reactive, barking and lunging? (With excellent management and modification, this might be acceptable if you have large animals – but it’s not acceptable if you have small animals.)
[D] Go into predator/stalking mode, or crouch, with a hard stare? (With excellent management and modification, this might be acceptable if you have large animals – but it’s not acceptable if you have small animals.)
A CHALLENGING QUEST
It’s been eight years since my husband and I have been closely affiliated with a shelter. Two years ago, in the same year, we lost our last two shelter adoptees to old age and cancer.
Our current dogs are not shelter alumni; we were unable to find the dogs we wanted through any of our local shelters or rescue groups. After lengthy searches we adopted one from a rescue group in New York (we live in Maryland) and the other was privately adopted; he was being rehomed through Craigslist. Now we can better empathize with the struggles of dog lovers to find good candidates for their own families.
Even so, scarcity isn’t a good reason to be less than scrupulous in your assessments. Remember, you are making a commitment of thousands of dollars for food and veterinary care, and countless hours of time spent with your dog over at least the next decade or more. Take your time! Good luck with your search.
Author Pat Miller, CBCC-KA, CPDT‑KA, is WDJ’s Training Editor. She lives in Fairplay, Maryland, site of her Peaceable Paws training center. See page 24 for information about her books and courses.
Jessie touches Woody's foot and he instantly looks at her with a happy "Where's my chicken?" expression: at this point, the touch on his foot elicits the desired happy conditioned emotional response (CER). She feeds him several bits of chicken, then stops touching his foot and simultaneously stops feeding the treats to him.
1. Determine the location of touch your dog can tolerate without reacting fearfully or aggressively. Perhaps it’s her shoulder, perhaps her elbow, or maybe just above her paw. She should be a little worried, but not growl or try to move away. This is “below threshold” – the emotional state where we want her to remain for all this work.
2. With your dog on leash, touch her briefly and gently at the spot where she is slightly below threshold – aware of your touch and somewhat concerned, but not highly concerned. The instant your dog notices your touch, start feeding her bits of chicken, non-stop. After a second or two, remove the touch and stop feeding the treats.
3. Keep repeating steps 1 and 2 until touching your dog at that location for one to two seconds consistently causes your dog to look at you with a happy smile and a “Yay! Where’s my chicken?” expression. This is a conditioned emotional response (CER); your dog’s association with the brief touch at that location is now positive instead of negative. Note: Feed the treats whether or not your dog displays the desired CER. The happy CER is a product of this process, but you don’t wait for it to happen each time.
4. Now increase the intensity of the stimulus by increasing the length of time you touch her at that same location, a few seconds at a time, obtaining the desired CER at each new touch and continue to feed for the duration of the touch. Do several repetitions of two to four seconds, until you get consistent “Yay!” looks, then several repetitions for four to eight seconds, then several four eight to 12 seconds, etc., working for that consistent CER at each new duration of your touch.
5. When you can touch your dog’s body at that spot for any length of time with her in “Yay” mode, begin to increase the intensity of stimulus again, this time by increasing the duration of your touch, then the amount of pressure, before moving your hand to a new location very slightly lower than the spot you were previously touching. I suggest starting at your initial touch location and sliding your hand to the new spot, rather than just touching the new spot. Continue with repetitions until you get consistent CERs at the new location.
6. Continue gradually working your way down to your dog’s paw, an inch or two at a time, getting solid CERs at each spot before you move closer to the paw.
7. As you work your way down the leg, be sure to add duration and pressure at each step before proceeding; each is a separate step in the CC&D procedure.
8. When you can touch, grasp, and put pressure on the paw, add lifting the paw, very slightly at first, then more and more, as you achieve the desired CER with each increase in lift. Then repeat the process with each leg. The other legs probably won’t take as long, but still, go slowly and be sure to achieve the happy CER with each step.
9. Did you think we were never going to get to the nail grinding part? We’re almost there! Start the process over again, this time with the nail grinder (or clipper) in hand. Show the tool to your dog at a sub-threshold distance until you achieve consistent CERs, then gradually move it closer (CERs at each step!) until you can touch the tool to her nail. Gradually increase the duration of the contact with her nail, and feed her a treat, again and again, until the appearance of the nail trimmer elicits a “Yay!” response. Then counter-condition the sound of the grinder (or the clipper action, by squeezing the clippers), starting again at a distance and gradually moving closer as you achieve consistent CERs at each step.
10. Go through the whole touch sequence again, this time with the trimming tool in your hand, also touching her with the tool, then again while you turn on the grinder or squeeze the clipper. Remember that you are still feeding yummy treats and obtaining the desired CER throughout the whole process. When you can hold her paw and use the tool right next to her nail with a happy response, grind or clip one nail, feed lots of treats, and stop. Do one nail a day until she’s happy with that, then advance to two nails at a time, then three, until you can grind or clip all her nails in one session.
The more complex the stimulus, the more successful the dog’s avoidance or aggressive strategies have been, and the more intense the emotional response, the more challenging it is to modify a behavior. Take your time. Be patient. A few more weeks – or months – of long nails isn’t the end of the world, and the result – a dog who willingly participates in the nail trimming procedure – is well worth the effort.
Casfuy's Two-Speed Pet Nail Grinder comes with Ni-Mh batteries that can be charged in three hours via a WSB cord (included)
There are dozens of grinding tools on the market – products specifically for trimming dogs’ nails, as well as rotary tools designed for woodworking or other projects. We polled a dog trainers’ group – people who habitually trim their own dogs’ nails – about the type and models of grinders they like best: Which products consistently get four tidy-nailed paws up for usability and effectiveness?
The consensus was that while the dog-specific rotary grinders are quieter, they take much longer to reduce the dogs’ nail length, especially on breeds with thicker nails. However, a few people said they find the grinders branded for use on dogs to be useful when initially training young or fearful dogs to tolerate nail trimming or for small breeds with thinner nails.
ENTRY-LEVEL DOG-SPECIFIC GRINDER
A quick search on Amazon reveals dozens of dog-specific nail grinders to choose from. Most all of them have a low-profile plastic guard covering the grinding bit. The plastic guard has a cut-out area that exposes just a small portion of grinding surface, and this is where you position the nail.
While I like that the presence of a guard appears to prevent the hair of a dog with a long coat (or the human operator’s hair) from accidentally getting wrapped around the quickly spinning tool head, it does seem to require better aim to get and keep the nail aligned with the cut-out. We noticed the guard on some products is removable in order to accommodate larger nails or for faster filing.
A good entry-level pet-specific grinder is the best-selling Casfuy Upgraded Professional Two-Speed Pet Nail Grinder, which sells on Amazon for $30. Note that the two speeds are both relatively low: 7,000 and 8,000 revolutions per minute (RPM).
A pet-specific grinder might be a nice addition to your toolbox, if you’re working with a breed with thin nails, or young, small, or fearful dogs, or you’re brand new to grinding and don’t want to start with a higher-power tool. If your dog has thick nails and/or you feel confident you can safely handle more power, it’s worth stepping up to a multi-purpose rotary tool.
HOBBYIST’S ROTARY TOOLS
When it comes to rotary tools that are not made specifically for pet nails, our panelists agreed on a top pick: The Dremel 8050 Micro. This grinder runs on an 8-volt rechargeable lithium battery. The tool features five variable speeds ranging from 5,000 to 25,000 RPM. Note that 5,000 RPM is too slow to accomplish much grinding and that 25,000 RPM will get the nail too hot too quickly. Overall, this product is quieter than older models – a plus for working with dogs.
Three features help give the 8050 its top ranking:
✓ The LED light that’s built into the tool’s nose cap (this illuminates the nails as you work – brilliant!).
✓ The docking station that keeps the tool fully charged and ready for use.
✓ If caught on something, the tool automatically stops.
If your grinder doesn’t have an automatic stop feature in case of a tangle, you must keep your own and your dog’s hair out of the way of the spinning tip. A baby’s sock with a hole in it protects your dog as well.
This last point is especially important when working with long-coated dogs or if you have long hair. (Pro tip: If your dog has hairy feet, try snipping a tiny hole in the end of a baby sock or nylon stocking. Cover the paw with the sock or stocking and use it to keep the dog’s long hair at bay. Don’t forget to pull your own long hair back, too!)
Dremel also offers a clear plastic “nail guard” attachment that clips onto a variety of its rotary trimmers. The guard is said to help achieve a 45-degree angle for trimming, manage nail dust, and hold a long-haired dog’s fur out of the way. If you already have a Dremel but aren’t comfortable using it, the Pet Grooming Nail Guard might make for nice “training wheels.” The guard is sold individually as the “AT01-PGK Pet Grooming Nail Guard,” but costs almost as much ($33!) as a kit that includes the guard and a Dremel 7760 rotary tool ($47 on Amazon.com). Get the kit if you don’t already have a rotary tool and like the idea of using a guard.
While many people visit a vet or groomer for their dogs' nail care, pandemic-induced restrictions have limited the availability of this option. So it's even more important to learn how to (and stay in the habit of) trimming your dog's nails yourself.
Maybe it’s the telltale click-clack as your dog moseys across the kitchen floor. Or the unmistakable and often painful raking sensation when she jumps up to greet you. Or maybe it’s when you’re lounging together on the couch and you realize your dog’s nails have grown so long, you’re not sure if you should trim them or see what they’d look like if painted a sizzling shade of fire-engine red!
Whatever prompts you to notice that your dog’s nails need attention, good for you. Nail care is important, and it’s often overlooked by owners who either aren’t sure how to do it, are afraid to trim nails themselves, or can’t quite get their dogs to go along with the program. If this describes you, we can show you how to do it most easily and how to get your dog to not just cooperate, but to willingly volunteer for a trim.
GRIND AWAY
The Benefits of DYI Nail Trims
There are many benefits of do-it-yourself dog mani-pedis, especially when you take the time to teach your dog to cooperate during the procedure by slowly and carefully desensitizing and counter-conditioning first. (See “A Counter-Conditioning Protocol for Nail Trimming” on page 5.) Some of the DYI benefits include:
• Improved health. Walking on long nails can affect how the dog moves and potentially contribute to the development of orthopedic problems, such as arthritis, later in life.
• Decreased stress. Teaching your dog to calmly tolerate a nail trim prevents stress and, potentially, fear-based aggression.
• Increased safety. The dog is less likely to be injured as a result of active resistance or panic-induced flailing, and you (or your vet or groomer) are less likely to sustain a bite.
• Body awareness. Time spent trimming nails is also the perfect opportunity to familiarize yourself with your dog’s physical topography. Regularly getting your hands on your dog – beyond basic petting – is a great way to quickly recognize changes that could indicate health problems.
• Financial benefits. The cost of professional nail trimming adds up over time!
There are two main ways to shorten nails: clipping with either a guillotine-style or a scissor-type clipper and grinding with a rotary tool such as a Dremel or a similar product designed specifically for grinding dog nails.
Between the two methods, many groomers (and I) prefer using a rotary nail-grinding tool, even though many dogs need to be desensitized to the sound and the vibrating sensation. The biggest advantage of using a nail grinder over clippers is that with clippers, if you cut off too much – either because you misjudged how much to cut, or the dog wiggled just as you squeezed the handle – you’re more likely to “quick” the nail by mistake. (“Quicking” a nail happens when you cut into the blood supply of the nail. It can be painful and, as a result of the yelp and reflexive action that the pain elicited from the dog, traumatizing for both the dog and the person doing the nails.)
In contrast, grinding the nail involves high-speed filing where the excess growth is ground down incrementally but quickly, as long as the tool is in contact with the nail. You can “quick” a nail by going too short with a grinder, too, but in our experience, you have to work harder to do so.
The other advantage of grinding vs. clipping is how the high-speed filing makes it easy to round off the tip of the nail, whereas clipping often leaves sharp edges. If your dog tends to paw at people for attention, this can be problematic until the nails naturally wear down into a more rounded shape.
We’ve published a number of articles in the past about clipping a dog’s nails; what follows here is all about using a grinder instead.
POSITIONED FOR SUCCESS
Author/trainer Stephanie Colman has taught her Golden Retriever, Saber, to relax on his back between her outstretched legs, which cradle and support him. It’s a great position for trimming his nails, as well as checking his paws for foxtails or other burrs, and giving belly rubs and face and chest massages.
It takes a little practice to figure out what position is most comfortable for you and your dog during the nail trim. Both of you on the floor? Him on the couch and you on the floor? On a grooming table? Some people find it easiest to trim the dog’s nails when he is laying flat on his side.
I find it easiest to sit on the floor, legs outstretched, with my dog on his back and cradled between my legs. I find this allows for the most comfortable angle of approach to grind the nails, and especially for rounding the edges, as I like to round up from the bottom of the nail. I teach and build value for this position early in my dogs’ lives, and we use it often – it’s an opportunity for quiet massage and “together time” – not just something we do when it’s time to trim nails.
No matter what position you use, don’t forget to first build a positive association with simply being in that position and having his paws handled before you add any of the steps that involve trimming nails. I feel strongly that all dogs should be taught to accept all the different behavioral pieces of a nail trim regardless of whether you will do nails yourself or if you plan to send the dog to a vet or groomer for routine trims.
It’s wise to “assume the position” often – for praise, treats, and calm petting – to help keep your dog from learning that your request for that particular position always accompanies nail trimming, in which case you may find your dog becomes reluctant to cooperate.
READY TO GRIND
The goal of nail trimming is to shorten the dog’s nails so that they don’t quite touch the ground when she is standing on level ground; she should be able to walk across the kitchen floor without a tap, tap, tapping sound. Nails that touch the ground will push the toes out of their natural position as the dog stands and moves; the longer the nails, the more displacement the toes will experience.
Remember, the innermost core of the nail consists of a vein and nerve, usually referred to as the “quick.” The longer the nail, the farther toward the tip of the nail the quick will extend. If your dog’s nails are far too long, it will take a lot of sessions of removing tiny bits of nail at a time to gradually return them to a healthy length without cutting into the quick, hurting the dog, and causing the vein to bleed (called “quicking” the nail).
Diamond grinding tips for rotary grinders are more expensive than sandpaper bands, but they grind more smoothly and don’t wear down quickly or need frequent replacement like sanding bands do, making them the preferred grinding tip of many professional groomers.
Fortunately, taking tiny bits off at a time is exactly what rotary grinders are best at! Frequently removing the excess nail a millimeter at a time will help the “quick” recede back toward the base of the nail. For very long nails, see if you can fit a few minutes of nail grinding once a week. It might take months of this to get the nails to a short and strong condition, but if you stick with it, your dog’s feet and legs will be much healthier for it. Once your dog’s nails have reached an appropriate length, just one or two short sessions of grinding each month should maintain them.
A few final tips:
* Don’t grind on any one nail for more than a second or two, as the friction creates heat, causing a burning sensation. Touch the grinder to the nail for one or two seconds and pull it away – a grind-release, grind-release pattern.
* To maintain the effectiveness of the grinder, be sure to replace the sandpaper-like sanding band once it’s worn. Replacement bands are inexpensive – about $6 for a package of 6 – and can be purchased through many online pet-supply stores.
* Using a diamond bit (instead of sanding bands) helps reduce the noise and vibration of grinding. These bitsare more expensive (anywhere from $20 to $20) but they last a long time.
With a little product research and some training and practice, you, too might soon find yourself a member of the rotary club.
Stephanie Colman is a writer and dog trainer in Southern California. She works in the puppy department at Guide Dogs of America, helping to recruit and manage volunteer puppy raisers.
Quick! What To Do About Bleeding
Whichever tool you use to trim nails, don’t get started without having some styptic powder on hand.
Styptic powder is used to quickly stop any bleeding that will occur if you accidentally cut into the nail’s blood supply. It’s an anti-hemorrhagic agent that works by constricting tissue to seal injured blood vessels.
Failing to have the powder nearby when you start nails is a great way to simulate a crime scene; if you have a “whoops!” moment when trimming your dog’s nails and have to go into the other room to get the powder, you can be sure your dog will leave a bloody trail – either following you or trying to run and hide from you!
Styptic powder is sold in a variety of containers with various applicators that are supposed to make it easier to get onto a cut nail quickly. Most commonly, however, it comes in a small jar. Some people tap some of the powder into the palm of their hand and then press the cut nail into the powder in their hand. I like to keep a little dish of water nearby so I can wet my finger without needing to lick it, especially during these pandemic times, where I’m being extra mindful of keeping my hands off my face in general. I coat my wet finger with a generous layer of styptic powder and press the powder directly onto the affected nail tip. I give a little tap to help pack the quick with powder.
Reapply as needed if the nail continues to bleed through the first layer of powder. If needed, you can temporarily occupy the dog with a favorite chew bone to prevent him from smelling and then licking the nail, re-starting the bleeding.
No styptic powder? In a pinch, cornstarch also works.
If the bleeding hasn’t stopped within 20-30 minutes, contact your vet, as that can be a possible sign of clotting issues.
Every month, it seems, we have an opportunity to share with you another pandemic-inspired article. This month, it is Stephanie Colman’s piece on “do-it-yourself” nail trimming. It’s important that your dog’s nails stay trimmed to a healthy length, whether or not your favorite grooming shop is open. Stephanie offers tips on equipment, positioning, and what to do if you accidentally cut or grind a nail too short and it starts to bleed. If your dog isn’t cooperative, check out the instructions on page 7 from WDJ’s Training Editor, Pat Miller, about how to counter-condition and desensitize your dog to nail trims.
We’ve included two articles about adopting dogs in this issue. If you’re looking to add a canine family member to your household, read them both!
Starting on page 8, Pat also shares her expert advice about how to identify and choose a dog who will fit well into your household and/or family. Pat’s descriptions of the specific behaviors that would indicate a sound adoption candidate are so incredibly helpful. I’ve volunteered for a long time at my local shelter and have witnessed countless would-be adopters meeting dogs that they were considering adopting, and I can honestly say that most of them don’t have a clue about what they are seeing when they interact with the dogs they think they want.
Trainer Kathy Callahan, author of the most moving dog book I’ve read in years (101 Rescue Puppies: One Family’s Story of Fostering Dogs, Love, and Trust), contributed a companion piece to Pat’s article. As someone who fosters homeless puppies for a few different rescue groups, Kathy loves to see puppies get adopted – but as you will see on page 13, she warns against any family casually adopting littermates on the spur of the moment. A multiple-puppy adoption can work out, she says, but it takes a lot of planning and effort.
Kathy’s article made me curious: Only once in all the years that I have raised foster puppies for my local shelter was I informed that an adopter wanted to adopt two of “my” puppies – and they were Great Danes. I was horrified that my shelter allowed this to happen and certain that two of the big galoots were going to be way too much for a family that had come to the shelter planning to adopt just one. Some time ago I posted an old video of my young dog in his “Fun Uncle” role, playing with that litter of puppies, and someone I know had commented that they knew someone who had adopted two of those pups. Afterreading Kathy’s article, I tracked down the adopter and the story. I was thrilled to find out that, four years later, they are still firmly embedded in their adoptive family. Yay!
Last week, I mentioned that there were a number of people coming to help locally with the emergency animal shelters established here in Butte County, California, where the North Complex West Zone fire, formerly known as the Bear Fire, has killed 15 people, burned at least 750 homes, and displaced thousands.
The fire was originally started by lightning storms on August 18. Locally, it was controlled and extinguished, but in a neighboring county, it burned in remote, mountainous areas until September 8, when it re-entered our county, driven by a ferocious windstorm. The wind pushed the fire more than 30 miles in the direction of the town where I live, Oroville, California, burning through the small town of Berry Creek and other even smaller remote communities. Within just a couple of days, the existing facility that can shelter small animals in emergencies such as this was holding a couple hundred dogs and cats.
I know this is just one fire among many burning across the western United States right now, so I’m even more humbled by the fact that volunteers have arrived from far and near to help the displaced and evacuated animals in my community.
Hundreds of dogs, cats, rabbits, birds, and smaller pets, and dozens of horses, llamas, pigs, sheep, goats, and chickens and other barn yard birds are being sheltered in three different locations in my town. Caring for them are a few animal control officers and dozens of volunteers. Many of the animals are considered “stray,” having been brought to the shelters by first responders on the fire lines, or by citizens who found them running loose as they themselves evacuated from the fires. Others were brought to the shelters by their owners, who have either lost their homes or are being kept from their homes by road closures in the area where the fire is either still actively being fought, or where the damage from the fire and firefight have rendered the area unsafe (downed power lines, trees fallen or falling across the roads, roads damaged by bulldozers, etc.).
As with the infamous Camp Fire of 2018, it’s expected that it will take weeks, if not months, for most of the displaced animals to be identified and/or picked up by their owners. Some may be surrendered to the county animal control, if their owners have no place to keep them.
Once again, our local animal rescue group NVADG leads the rescue efforts
Much of the heavy lifting is performed by volunteers belonging to a local group, the North Valley Animal Disaster Group (NVADG, pronounced as “NAV-Dag). When animals are affected by a local fire or other disaster (including floods, animal trailer rollovers, horses who have fallen off cliffs, etc.), county animal control officers contact and activate NVADG. Experienced NVADG volunteers set appropriate actions into motion; in this case, volunteers immediately went to work opening buildings lent to NVADG by the county to use for this purpose, and started setting up crates and an intake process to identify and track each animal brought to the shelter. NVADG volunteers care for the animals, with supervision and oversight provided by county animal control officers.
It’s a rough fact that the process of keeping these animals safe is highly stressful for the sheltered small animals, no matter how good their keepers’ intentions for them are. Cats are in cages with small litterboxes; for the most part, dogs are kept in large wire crates. (Especially huge dogs, such as the Anatolian livestock protection dogs that we are sheltering, or large dogs who prove to be particularly hard to keep enclosed in a wire crate, are kept in small pens within the temporary shelter buildings.) They are taken out of the crates and walked about three times a day – which sounds (and is) incredibly minimal, and yet requires an army of volunteers to accomplish.
I’d like to mention a few of the organizations that have sent workers or volunteers to our shelters from out of this area. I’m honored to have worked alongside many of them.
IFAW
Image courtesy of IFAW
First on the scene from out of the area were folks from the International Fund for Animal Welfare (IFAW, pronounced eye-faw). The organization describes itself as a global non-profit helping animals and people thrive together. They work in more than 40 countries across the globe, partnering with other animal welfare groups and even just concerned citizens who are trying to help animals in their communities. IFAW workers were a huge part of the response to the Camp Fire two years ago, and some of the same individuals who came here then returned to help us again.
IFAW workers flew into California on September 14, and immediately began setting up a second temporary shelter in a leased warehouse. Within a day, animal control officers started transferring “stray” animals from NVADG’s overcrowded site to the more spacious temporary facility. Some IFAW workers stayed on the new site, working alongside NVADG volunteers to care for the animals, while others went into the fire zone with search and rescue teams, looking for hurt animals and ones that had been left behind. These folks work 12- and 14-hour days while thus deployed, and are, to a single person, cheerful, hard-working, and driven to improve the care and treatment of animals in any way they can. Their expertise and guidance to local leaders is incredibly valuable.
Sonoma CART
I lived in Sonoma County, California, during my high school years and as a young adult, so I know that the differences between that county and this one could not be more stark. Sonoma County is wine country, home to lush redwood forests, grassy foothills grazed by dairy cows, an unbelievably gorgeous coastline along the Pacific Ocean, and affluent towns that are home to many urban tech workers. About 200 miles to the north and inland, Butte County is much more economically challenged, hotter, and drier. Butte County’s largest city is smaller than most Sonoma County cities; its total population is less than half of Sonoma County’s.
But they have one thing in common: They both experienced horrific destructive fires in the past three years. The 2017 Tubbs Fire burned in Napa, Lake, and Sonoma counties, but its worst devastation occurred in the city of Santa Rosa, where it killed 22 people and burned thousands of homes and businesses. Sonoma County Animal Rescue Team (Sonoma CART) was already in existence at the time of the fire, and its trained volunteers were instrumental in providing assistance to the animals affected by the Tubbs Fire. In the months and years after the Tubbs Fire, many Sonoma County residents joined Sonoma CART and took its training classes – and many have gone on to respond to calls for help during other California disasters. I’ve met eight or more members of Sonoma CART while working with dogs at the NVADG shelter during this fire, each of whom drove hours to get here, spent their own money to stay in local hotels, and labored for days in a row to feed and walk dogs and care for other animals.
At least one volunteer I worked with spent a week here, working 12-hour days. On her last day here, we shared some bonding moments over a blind, elderly yellow Labrador who needed some extra TLC, and she shared photos of her own senior Labrador, who had died not long ago. She also confided in me that she did this work in honor of her mother, who lost pets in a fire some years ago and “has never been the same since.” We both shed tears as she recounted her mother’s pain; with heavy smoke in the air, surrounded by displaced animals, we could only too keenly imagine losing our own beloved dogs.
Thank you, Sonoma CART, for sending such generous, open-hearted people to help us.
Red Rover
Image courtesy of Red Rover
This is another national organization who showed up during the 2018 Camp Fire disaster to help run the emergency animal shelters – and who has sent workers once again to provide our weary local animal control officers with some much-needed respite. Red Rover has more than 4,000 volunteers who have taken one or more training courses in emergency response for animals, and they help provide emergency sheltering assistance for animals displaced by natural disasters and rescued from other crises, such as puppy mills and hoarding situations.
Red Rover workers have been on the ground here for the past few days, and, I hear, more are due to arrive this week. The emergency shelters here will likely be operating for at least another month, if not longer, as so many people have no houses to take their pets home to, so the extra help is highly needed and will be appreciated.
After two weeks, many of us local volunteers are exhausted, or have given as much time as we can spare. Thank goodness for fresh boots on the ground! I’ve been working closely with a Red Rover worker who flew in from New York, who has been helping to run the NVADG shelter for the past few days, giving the NVADG volunteer leaders who had been operating the shelter for the past two weeks a chance to sleep and catch up on their regular-life duties. She’s been amazing and cheerful, even in the face of poop-splattered crates and a too-thin list of local volunteers arriving for the 7 am dog walking and crate-cleaning shift. Devon Krusko, thank you!
Image courtesy of Red Rover
Find an “animal rescue” class and take it!
If you ever had a hankering to pitch in to help animals in (or near to) a disaster zone, check out the national organizations IFAW and Red Rover. Both offer courses to help people understand how to work in conjunction with professional rescue workers in an “Animal Incident Command System Matrix.” And if fires or floods or other natural disasters commonly affect or displace people and their pets in your local area, look for a local organization such as NVADG or Sonoma CART to train and work with. Helping feels a whole lot better than just watching and worrying from afar.
Did you know that there are unflavored heartworm preventative chews available, as well as other forms of preventatives? I didn’t either, until recently.
Pixel, my sister’s dog, was just diagnosed with a gastrointestinal disease that was causing inflammation of her intestinal tract and malabsorption of food. Fortunately, this condition was quickly resolved by changing Pixel’s diet to a novel protein and eliminating any foods with beef, pork, or chicken and she is now thriving. Then it became time to administer her monthly chewable heartworm preventative. My sister hesitated: The chewable preventative medication that she ordinarily used to protect Pixel was flavored with chicken, which Pixel couldn’t have. Fortunately, there are alternatives, and Pixel’s veterinarian was happy to change Pixel’s prescription to one of these.
Heartworm disease is a serious and potentially fatal condition caused by Dirofilaria immitis, a parasitic roundworm that is transmitted to dogs through the bite of a mosquito. Unfortunately, canines are natural hosts for the parasite, and once it infects a dog’s body, the larvae mature into adults, mate and reproduce, with the adult forms of the heartworm residing in the heart, lungs, and associated blood vessels. Heartworm disease can cause lasting damage to a dog’s body and have a long term effect on health and quality of life. Heartworm disease has been diagnosed in all 50 states; risk levels for contracting the disease vary and are difficult to assess. Accordingly, prevention is usually necessary in most areas. Heartworm medications do not actually prevent the transmission of the heartworm, but rather they act to destroy the larval stages of the parasite, preventing the development of the larvae into adult heartworms.
Prevention of heartworm disease is usually achieved by the monthly oral administration of a flavored chew, which is highly effective when administered correctly. Most oral heartworm preventives, however, contain a protein-based component for flavoring, usually pork, soy, beef, or chicken, in their formulation. Because many dogs suffer from food allergies and sensitivities or are undergoing food elimination trials (and flavorings can interfere with and affect the success of the trial), heartworm prevention in these cases should be changed to a non-flavored oral formula or topically applied product.
The monthly heartworm preventive HEARTGARD® (ivermectin) is available in an unflavored tablet form and does not include any food ingredients that may trigger an allergic reaction. A topical (applied externally to the body) heartworm preventative, such as Advantage Multi, Revolution, or Selarid, is another option, especially as this form completely bypasses the gastrointestinal tract.
There is a third option: ProHeart 6 and ProHeart 12 take the form of sustained released injections of moxidectin (this ingredient is also available as a topical) and provide protection from heartworm infection for six months and twelve months respectively. Its use in the U.S., however, still draws controversy over concerns regarding adverse effects (ProHeart 6 was taken off the market in 2004 because of safety concerns, but it was reformulated and returned in 2008; ProHeart 12 was approved for the first time by the FDA for use in the U.S. in July 2019). In other countries, both products remain on the market and are in use.
As always, consult with your veterinarian about your dog’s prescription heartworm preventative.
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.
This website uses cookies and other tracking technologies to offer you a better experience, personalize content and ads, and analyze our site traffic. Before proceeding, you agree to our Terms and that you’ve read our Privacy Policy. Update Settings
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.