
To continue reading this article or issue you must be a paid member. Sign in
Join Whole Dog Journal
Get full access to Whole-Dog-Journal.com – more than 4,000 articles – for just $20.
Join today and save 30% off our full price.

Subscribe
The best in health, wellness, and positive training from America’s leading dog experts


Heartworms are just what they sound like: worms, up to 14 inches long as adults, that develop and live within the blood vessels of the dog’s heart. Though they prefer the right side of the heart, in a severe infection, they also develop and live within the lungs or any major artery – wherever they can find room with access to blood.
Heartworm disease refers to the constellation of ill effects the dog suffers as a result of this population growing inside him. Heartworm disease has the highest morbidity and mortality of any insect-transmitted disease in the United States.
At one point, heartworm disease was considered a problem of certain areas (the Southeast is notorious for this), changes in climate, dogs being moved across state lines (for instance, dogs relocated from Louisiana after Hurricane Katrina), and changes in wildlife territories have all led to fluctuations in the distribution patterns of the disease. As a result, heartworm disease in dogs is no longer limited to particular parts of the country.
The good news is that with the advent of modern parasiticides and routine surveillance (testing for heartworms), heartworm disease can be prevented. If prevention is not taken and a dog becomes infected with heartworms, he can be treated for the infection – but the treatments can pose a risk to the dog. Prevention is the best approach!
Dogs become infected with heartworms through the bites of infected mosquitoes. A mosquito who has taken a blood meal from an infected canid (dog, coyote, wolf, fox) transmits heartworm larvae into the next canid it bites.
The microscopic heartworm larvae enter the dog from the mosquito’s mouthparts and begin a developmental journey that sees them progress through several larval forms and migrate into the dog’s bloodstream, looking for a hospitable place to attach and grow into adult worms.
The pulmonary arteries where the adult worms ultimately lodge become inflamed, dilated, and malformed, as the heart labors to push blood past the obstructing worms. Blood clots and aneurysms (a dangerously ballooning bulge in a blood vessel) can develop.
The heavier the heartworm “burden” – the more worms that the dog is infected with – the worse the dog’s symptoms and prognosis will be. Dogs can become infected with so many parasites that the heartworms can obstruct the flow of blood through the heart, leading to dilation and thickening of the laboring muscles of the right side of the heart. The thickened heart muscle is subject to disturbances in the electrical impulses of the heart, leading to arrhythmias.
If the worm population is unchecked, the heart becomes too distorted to function at all, and the dog can suffer right-sided heart failure. Or, “caval syndrome” may be observed, where the entire right side of the heart is filled with heartworms, interfering with closure of the tricuspid valve and impeding the flow of blood through the heart, leading to cardiovascular collapse.
As the heartworm infection progresses, the blood vessels of the lungs (pulmonary vasculature) become inflamed and unhealthy. This causes pulmonary hypertension (high blood pressure in the lungs). And as the worm-laden heart has to work harder, it becomes less able to pump blood throughout the body, driving the acquisition of oxygen and expelling carbon dioxide in the lungs. As this progresses, the dog becomes increasingly intolerant of exercise – or, in severe cases, any movement at all. The dog will develop a chronic cough that worsens over time, and the dog’s belly may become distended with fluid (ascites).
The heart, lungs, and even the kidney and liver eventually show signs of disease – all caused by the increasingly inefficient labors of the burdened cardiovascular system.
Caval syndrome is an uncommon but lethal condition in which a massive clot of worms suddenly obstructs the vena cava (a large vein that carries blood into the heart). This occurs when a dog has a heavy infection of adult heartworms and it leads to immediate, life-threatening shock. A dog will collapse, have pale gums, rapid heart rate, and fast, irregular breathing. Bloody urine can develop, and body temperature may be low.
There is only one successful treatment for this condition, and it is invasive and risky. It involves making a cut into the jugular vein and manually removing the clot of worms from the heart with long forceps.
Once enough worms are removed, the heart can pump efficiently again. This treatment requires general anesthesia while a dog is in a state of shock, as well as 1 to 2 days of hospitalization for recovery followed by adulticidal treatment. The prognosis is extremely guarded.
It usually takes at least a year before a dog, bitten by an infected mosquito, shows signs of heartworm disease – and it may take even longer. The symptoms that dogs may display as a result of their heartworm infection depend on a number of factors:
Early signs of a heartworm infection in dogs may be a mild cough or “slowing down” during exercise (exercise intolerance). You may notice that your dog becomes reluctant to run and play or tires quickly, particularly in the heat. A dog who is only lightly infected (with just one or two worms) may never experience worse symptoms than this.
However, dogs who have a heavier worm burden and/ or become repeatedly reinfected will suffer worsening and serious symptoms. Eventually, total failure of the right side of the heart occurs. Blood-tinged fluid may drip from the nose. Dramatic weight loss called cardiac cachexia can be noted. This is end-stage heart failure and successful treatment is difficult. At this stage, death is not far off.
To understand how best to prevent and treat heartworm infections, it helps to understand the life cycle of the heartworm.
The heartworm goes through several physical transformations in its lifetime and requires hosts of two different species to complete its life cycle: the mosquito and a mammal. The life cycle starts in an infected animal. If an adult male and a female adult heartworm are both present in a dog, they can produce microfilaria, a type of motile embryo. The microfilariae circulate freely in the infected animal’s blood and cannot develop any further unless they are sucked up into a mosquito through its bite.
The next stages of a heartworm’s development can take place only in the gut of a mosquito – weird, right? Once a mosquito ingests a blood meal laden with microfilariae, the microfilariae start to mature. Over a period of 10 to 30 days (average is about two weeks), the microscopic embryos develop through three larval stages – still very microscopic, but each distinct. If the mosquito bites another dog, any larvae in the third stage of development (called L3 larvae) exit the mosquito through its mouthparts and enter the dog. Only once the L3 larvae are in a mammal again can they develop further.
The larvae live and continue to develop in the dog’s subcutaneous tissue for about 50 to 70 days, in a stage called L4 – the fourth larval stage. Once that stage is complete, the larvae begin to migrate through the dog’s tissues, in search of the circulatory tract. Once they reach a blood vessel and enter the bloodstream, they become sexually immature adults. These juvenile worms move toward the heart and lungs, where they latch on and mature into sexually capable adults who can mate, so the females can produce viable embryos (microfilaria), starting the life cycle again.
This entire process, from the bite of the mosquito who takes the microfilaria from an infected dog, through the larval stages in the mosquito, through the larval stages in a new mammal host, to adulthood, takes a minimum of about six months.
It’s important to understand this cycle, as veterinary technology can prevent your dog’s infection, or, failing that, detect his infection in order to deliver a timely treatment, at specific times in the heartworm’s life cycle, and under specific conditions.
Heartworm preventative drugs belong to a class of medications called macrocyclic lactones. They have been in existence for about 30 years and are derived from the soil microorganism Streptomyces.
Macrocyclic lactones are used in both the treatment of human and animal parasitic diseases. These medications work by inhibiting nerve transmission within parasites, leading to their paralysis and death. They effectively kill the third-stage larvae that infected mosquitoes may have newly implanted in your dog, as well as the fourth-stage larvae that are developing under his skin.
These drugs do not kill any juvenile or adult heartworms that may already reside in the circulatory tract (though the drugs may weaken them). Once the larvae reaches the bloodstream, it’s too late for the preventative drugs to kill them. To be effective, the drugs must be administered between the bite of an infected mosquito and when the larvae reaches young adulthood. That’s why these drugs must be administered precisely on the schedule recommended by their manufacturers (monthly for many of the drugs, or according to label instructions).
| Heartworm Preventative | Active Ingredients | Form | Effective Against | Duration | Manufacturer |
|---|---|---|---|---|---|
| Advantage Multi | imidacloprid, moxidectin | topical | heartworms, adult fleas, sarcoptic mange mites, roundworms, hookworms, whipworms | 30 days | Bayer |
| Heartgard | ivermectin | oral | heartworms | 30 days | Boehringer Ingelheim |
| Heartgard Plus | ivermectin, pyrantel | oral | heartworms, hookworms, roundworms | 30 days | Boehringer Ingelheim |
| Interceptor Plus | milbemycin, praziquantel | oral | heartworms, hookworms, roundworms, whipworms, tapeworms | 30 days | Elanco |
| IverHart Max | ivermectin, pyrantel, praziquantel | oral | heartworms, hookworms, roundworms, tapeworms | 30 days | Virbac |
| IverHart Plus | ivermectin, pyrantel | oral | heartworms, hookworms, roundworms | 30 days | Virbac |
| ProHeart 6 | moxidectin | injection | heartworms | 6-12 months | Zoetis |
| Revolution | selamectin | topical | heartworms, fleas, ear mites, ticks, sarcoptic mange mites | 30 days | Zoetis |
| Sentinel Flavor Tabs | milbemycin, lufenuron | oral | heartworms, hookworms, roundworms, whipworms, fleas | 30 days | Virbac |
| Sentinel Spectrum | milbemycin, lufenuron, praziquantel | oral | heartworms, hookworms, roundworms, whipworms, tapeworms, fleas | 30 days | Virbac |
| Simparica Trio | sarolanar, moxidectin, pyrantel | oral | heartworms, ticks, fleas, roundworms, hookworms | 30 days | Zoetis |
| TriHeart | ivermectin, pyrantel | oral | heartworms, hookworms, roundworms | 30 days | Merck |
| Trifexis | spinosad, milbemycin | oral | heartworms, fleas, hookworms, roundworms, whipworms | 30 days | Elanco |
Most dog owners have had their dogs tested for heartworm infections, but many are unaware of the limitations of these tests.
The most sensitive and readily available antigen detection test is a snap test that can be conducted in your vet’s office. A blood sample is drawn, mixed with a conjugate solution, and applied to the test. Results are available within 10 minutes.
The most common heartworm tests used by veterinarians detect the antigens that are released by adult female heartworms into the dog’s bloodstream. In most cases, antigen tests can accurately detect infections with one or more adult female heartworms.
Currently there are no USDA-licensed serologic tests that can detect male heartworms. This means if a dog, by chance, is infected with only male heartworms, the test won’t catch it. And if a dog is infected, but the heartworms have not yet reached adulthood, the test won’t catch it.
Also, if a dog is infected with just one or two adult female heartworms, the tests will detect antigens produced by this tiny female population only 60% to 70% of the time. The dog may test negative or inconsistently positive.
In addition, according to Michael W. Dryden, DVM, MA, PhD, of the Kansas State Veterinary Diagnostic Laboratory, recent studies have documented that antigen tests may not test positive in up to 7% of dogs due to the occurrence of “antigen-antibody complexes” that are formed in the dog’s blood.
So, to counter these rather sobering testing statistics, in an ideal world, puppies would be started on heartworm preventative medication at their first veterinary visit, and receive their first heartworm tests at or just before a year of age. Since tests cannot detect heartworms before the heartworms are 6 to 7 months of age, there is little reason to test much sooner. (That said, if I was looking at a rescued dog of indeterminate age who lived primarily outside before rescue, especially in a warm climate where mosquitoes are active year-found, I would test him sooner.)
Your veterinarian might also look at a blood sample under the microscope. The microfilariae are easy to detect, as the active embryonic larvae are much bigger than blood cells. They also “whip” from side to side. A positive antigen test and the presence of microfilaria definitely means that a dog has a heartworm infection.
If the antigen test is positive, but no microfilariae are detected, then a second heartworm test should be conducted to confirm the positive finding. Treatment for the infection should not be started until the positive has been confirmed.
If a dog tests negative but has symptoms compatible with heartworm disease and hasn’t been taking prevention, then more extensive testing is necessary. This includes a blood smear to look for microfilaria as mentioned above. “Heat fixation” is a newer test, conducted by outside laboratories, that can dissociate the antigen-antibody immune complexes, unbinding any heartworm antigen present so that it is detectable by the antigen tests.
If you choose to import a dog from another state, make sure that he has been thoroughly examined and tested for heartworms – both so he can be treated promptly and to eliminate the possibility that he provides a new local reservoir (host) for heartworms in your area.

Some breeds of dogs, particularly white-footed herding breeds such as Australian Shepherds and Collies, are known to have a deficiency of P-glycoprotein. This is known as the multi-drug resistant mutation (MDR1). Dogs with this mutation are unusually sensitive to certain classes of drugs including macrocyclic lactones (MLs).
However, studies have shown that at the standard preventive doses, MLs are safe in all breeds. This is why it is important to use the canine products rather than trying to dose large animal products. The vast majority of toxicities in MDR1 mutation dogs were caused by overdose of large animal products or accidental ingestion of too much medication.
If a heartworm infection is confirmed, the next step is determining how advanced the disease is. This can include x-rays of the chest to look at the dog’s heart size, lungs, and blood vessels.
Some veterinarians will also conduct an electrocardiogram (ECG) to evaluate the heart rhythm for abnormalities, as well as an echocardiogram – an ultrasound of the heart. This will determine if the heart is enlarged, and heartworms will show up on the echo as bright white lines. Knowing the severity of disease can predict the likelihood of complications from treatment.
Dogs with minimal cardiovascular changes have a good prognosis. The presence of heart failure, significant lung changes, and caval syndrome complicates treatment significantly.
The treatment of heartworm infections has advanced significantly in recent decades.
Initially, oral prevention such as milbemycin is administered for two months, along with doxycycline. The oral prevention kills the larval forms and any circulating microfilariae that may be present. (The microfilariae can’t develop into heartworms in your dog – but you don’t want your dog to be a host for any stage of the heartworm life cycle!)
Doxycycline is an effective antibiotic against Wolbachia, a parasite harbored within the heartworm. By killing the parasites in the heartworms, the heartworms themselves are weakened. When administered as part of therapy, doxycycline lessens the complications of infection.
At two months (day 60), it’s time to administer melarsomine (Immiticide), the drug that actually kills the adult heartworms. The drug is given as an injection deep into the epaxial muscles along the spine on days 60, 90, and 91. During treatment, extremely strict crate rest with or without sedation and close monitoring are required.
A dog’s prognosis depends on the severity of infection at the time of treatment, as well as the management of the dog during the treatment period. As the worms die, they decompose in the bloodstream. If a dog exercises enough to elevate his heart rate, severe complications such as worm or pulmonary embolism (blood clot) leading to respiratory distress and collapse can occur. Treatment for embolism is hospitalization for oxygen therapy and steroids to decrease inflammation in the lungs. Many dogs will do well if this is caught and treated quickly. But it can’t be repeated enough: It’s critical to strictly control the dog’s activity while he undergoes treatment for heartworm infection.
Other helpful medications include steroids to reduce inflammation as the worms die, as well as pain medication to alleviate discomfort caused by the deep intramuscular injection of melarsomine. Sedatives may be needed to keep a dog rested, calm, and exercise-restricted. According to the American Heartworm Society, “A pivotal factor in reducing the risk of thromboembolic complications is strict exercise restriction.” An antihistamine may also be administered to reduce the risk of anaphylaxis.
Monthly preventative medication is the most effective way to prevent canine heartworm infections, but here are a few more:
• Eliminate sources of standing water in your dog’s environment. Ask your local or county mosquito abatement manager what you can do to control mosquitoes.
• Minimize your dog’s time outdoors at prime mosquito feeding hours (dawn, dusk).
• Make sure to administer preventions monthly and use only those specific to canines. Do not use large animal products as it is easy to mis-dose these and cause toxicity.
• If any doses of preventative are missed, contact your veterinarian to discuss appropriate next steps.

The so-called “slow kill” method of treating a heartworm infection consists of a monthly dose of heartworm preventative medication only; no adulticidal medications are used. Remember, the preventative medications kill any circulating microfilariae as well as any L4 forms of the parasite. But these medications don’t quickly or reliably kill the adult heartworms that damage the dog’s circulatory and pulmonary systems, though they do weaken the adult worms and shorten their life span. The result is that the heartworms may take as long as two years to die, as opposed to a couple of months.
A 2004 study examining the efficacy of the slow-kill method determined that nearly 30% of dogs still tested positive on a heartworm antigen test after 24 months of monthly heartworm prevention.
Finally, the slow-kill method may not destroy a subpopulation of worms that are resistant to the medication, leading to a worse infection that cannot be treated with macrocyclic lactones.
A slow-kill protocol is inexpensive in terms of money spent by the dog’s owner, but very costly in terms of the dog’s health. Dogs being treated in this way must be strictly rested to prevent the risk of pulmonary blood clots caused by the breakdown of dead heartworms. As long as the heartworms are alive, pathologic changes to the lung and heart tissue continue, and this damage is usually permanent.
In contrast, the conventional treatment has been shown to clear heartworm infections 98% of the time – and within a couple months of starting the treatment protocol.
Heartworm disease is a serious, often fatal syndrome. Prevention is simple! Administer monthly prevention to protect your dog, minimize mosquitoes in your environment, and work closely with your veterinarian to develop a healthy lifestyle.

Are you aware every single time a potentially L3-laden mosquito bites your dog? Of course not; no one is. That’s why the preventative drugs are delivered monthly – to kill any larvae that may have been deposited in your dog in the last month, before any of them can develop into mature heartworms and take up residence in your dog.
With the understanding that heartworm infections start with mosquito bites, some dog owners limit the administration of heartworm preventative drugs to seasons when they can witness the presence of mosquitoes; for example, they may stop giving preventative drugs in fall and winter. Some owners feel their dogs are so rarely outdoors, or that their climate is so mosquito-free, they don’t need to give their dogs heartworm prevention.
As a veterinarian, I’ve heard these reasons and more. Some of my clients have told me that they live in an area with a particularly low endemic rate of infection or that they’ve never personally experienced heartworm in previous pets. They may also have concerns about the cost of preventative drugs or fear adverse side effects from the administration of preventives.
According to the American Heartworm Society, “Heartworm disease has been diagnosed in all 50 states, and risk factors are impossible to predict. Multiple variables, from climate variations to the presence of wildlife carriers, cause rates of infections to vary dramatically from year to year—even within communities. And because infected mosquitoes can come inside, both outdoor and indoor pets are at risk.”
With rare exceptions, all dogs should be on heartworm prophylaxis (preventative drugs) year-round. Puppies should be started on these medications as early as possible. There are oral, topical, and injectable options on the market, so administration has never been easier. These are weight-based medications and will be adjusted as your dog grows.
Many prescription heartworm preventions also treat intestinal parasites such as roundworms and hookworms. Some also prevent whipworms and tapeworms. A few are now combined with flea and tick prevention. By administering these medications, you keep your pets healthy, as well as yourself and family members. Some intestinal parasites are zoonotic to people, including hookworms, tapeworms, and roundworms. Children are particularly susceptible.
To help you make the decision whether to administer heartworm medications, the American Heartworm Society website provides valuable insight on rates of infection in your state, as well as zoomed-in views of certain local areas. There are incidence maps available for the United States, helpful infographics, and even an area just for kids. Go to www.heartwormsociety.org.
There are many prescription options on the market, and your veterinarian will likely only carry some of these. Discussing your lifestyle and preferences with your veterinarian can help determine which works best for you and your dog. But you need to use something!


Suddenly, thanks to COVID-19, the whole world is asking the question that’s all too familiar to savvy puppy owners: “How likely is this experience to result in infection, and is this particular interaction worth it?”
There’s a stretch in puppyhood – up through around 4 months – when puppies are typically vaccinated several times but cannot be considered fully immunized against parvovirus and distemper due to the potential for maternal antibody interference. (For in-depth information about serial puppy vaccinations, see “Puppy Vaccines,” WDJ October 2016.)
Lamentably, a convincing swath of research has identified that exact same stretch of time as the almost magic (but fleeting!) period when pups are wide open to new experiences that will set them up for a lifetime of confidence.
The tension between those two scientific truths presents owners with a dilemma after bringing home an 8-week-old pup. Staying at home those first two months is the only way to keep a pup 100% safe from infectious disease – but doing that could well lead to debilitating behavioral issues down the road.
So what’s an owner to do?
My own complicated answer is that the safest all-around approach is to thread the needle, work hard to assess risk, and make educated choices. Happily, that just got easier thanks to COVID-19, which seems bent on supplying the dog world with more than its share of silver linings. Suddenly, the instructions that used to seem too tricky to follow are becoming second nature:
As a dog trainer who specializes in puppyhood coaching, I’m thinking COVID-trained people are going to find it easier to make the nuanced choices for puppies that will result in wonderfully confident, friendly adult dogs.
Parvovirus and distemper are two deadly canine illnesses that, thankfully, have effective vaccines. The catch? The shots are given in a series over the first months of the pup’s life, and you can’t be sure exactly when a shot will “take” and provide immunity. That’s why we need to approach the entire time period with caution.
Historically, veterinarians have advised owners to keep their pups at home until they were fully immunized. (Simply keeping your distance from other dogs isn’t good enough, because disease can lurk in the environment.) Over the past decades, however, the science has become very clear on how harmful it is for a pup to miss out on its prime socialization period. In fact, the American Veterinary Society of Animal Behavior (AVSAB, veterinarians who are board-certified in behavior) came out with an official statement in 2018 that says, in part:
“The primary and most important time for puppy socialization is the first three months of life. During this time puppies should be exposed to as many new people, animals, stimuli and environments as can be achieved safely … it should be the standard of care for puppies to receive such socialization before they are fully vaccinated.”
To read the full statement, click here.
While some vets still feel safer giving the black-and-white guidance to wait – after all, it’s much easier for clients to follow – most now advise careful socialization. “Make no mistake, parvo and distemper are still out there, in pockets, everywhere,” says Maine veterinarian, author and radio show host Dr. John Hunt. “But there should be a push for proper, safe socialization from weaning through 16 weeks.”

The consequences of a puppy’s lack of socialization during that key time frame can be heartbreaking. In fact, AVSAB points out that the number one cause of death for dogs less than 3 years of age is behavioral issues, not infectious diseases. In extreme cases, fearful dogs can become aggressive and bite; in some cases they may be surrendered to shelters or rescues, and sometimes are ultimately euthanized. It’s terribly sad – and often preventable. How? With a little “vaccine” called socialization.
From the moment puppies are born – and maybe even sooner! – the potential for learning about the world begins. The more positive interactions those pups have with novel sights, smells, sounds, people, and animals, the more they’ll confidently approach new things for the rest of their lives. The benefits that follow cannot be overstated: It means happy walks amid other dogs and people, easy hosting and gatherings with extended family, calm vet visits, and the delight of taking your friendly dog on vacation.
In contrast, if you wait to venture out of the home cocoon until all shots are complete, it may be too late. Starting at around 4 months old, biology tells a puppy that anything new and different might be a threat. You may have a dog who is forever skittish (or worse) around new people, other dogs, unfamiliar places. Until you live with a dog like that, you can’t understand just how sad and difficult it is. Everything is hard.
I foster litters of puppies, safely exposing them to everything that I can in their time with me. I’ve seen first-hand what happens when, after adoption, socialization comes to an abrupt halt, and the pup spends the next two months “safe” in her own predictable house. At the 6-month mark, the well-intentioned owners are devastated about their now-fearful pup, explaining, “It struck us that two months wasn’t very long to wait, and we thought we could just make up for it later.” Alas, biology disagrees.

There’s one thing everybody agrees on: The easy, first step of socialization is to make the most of the puppy’s time at home. If you work at it, even your own house can offer novelty.
Note: Be careful not to overwhelm your pup with this! The point is to help him learn that the world may be loud or unpredictable, but it’s always safe and can be a lot of fun. Go at your pup’s speed. If he seems worried – perhaps not taking treats, or revealing his tension by grabbing at them much more roughly than usual – increase the distance between the stimuli and the pup, and/or decrease the intensity of the stimulus.
* Don’t shield your pup from “scary” noises like the vacuum or leaf blower. Instead, seek out those experiences for the pup – but control the stimulus, using your pup’s reaction as a guide. Start at a distance and pair the stimulus with many small treats. If he becomes frightened, increase the distance between the stimulus and the pup. Ideally, he continues to cheerfully play and interact with you.
* Sit out front when it’s busy on your street and help your puppy enjoy passing trucks, bikes, strollers, or other dogs by offering tiny bits of chicken or cheese each time.
* Play dress-up! Have everybody in your household make a practice of wearing “strange” things: hats, masks, hoodies, big clumpy boots, backpacks. Keep your voices happy and light and playful. Got old crutches in the attic? Use them! You get the idea.
* Have pup walk on every possible surface in and around your house: carpet, tile, hardwood, grass, stone, dirt, yoga mat, cushion, wobbly cardboard box. Make it a fun game with – you guessed it! – treats or your puppy’s favorite toys.
* Use the radio, TV, and even specially designed doggy soundtracks to make sure your pup hears babies cry, young kids scream with delight, big men talk in deep voices, etc., and has a good time doing so.
* Make a point of inviting over every category of human you can: a nice preschooler, a grandmotherly neighbor, a super-tall guy. Even a three-minute visit makes a difference. Is the puppy nervous? Add distance, squat down, lower voices, add treats, be patient.
* Turn any visits from the plumber or electrician into a serendipitous socialization opportunity. Ask if they’d mind tossing your puppy a treat, or handing it over if the puppy is confident and curious.

Doing as much as you can at home is a wonderful start, but it can’t compare with getting your pup out and about. This is where your COVID learning kicks in. Be smart. Plan ahead. Minimize risk.
The first rule is easy: Avoid unknown dogs and the places they frequent. No dog parks, pet stores, or animal shelters until your pup is fully protected by that last vaccination.
Everything else falls in the “well, it depends” category, which means you have to put on your thinking cap. As you ponder each situation, think outside the box. How about bringing a blanket to cover the ground while you and pup sit at your local park, greeting people? Or expose your pup to new folks and sounds on your town’s Main Street by using a stroller or carrier, so pup can enjoy without paws touching the ground. (Get pup used to it at home, first, so the stroller itself isn’t scary!) Just one positive 15-minute visit like these in this key time period can dramatically shape a pup’s view of the world. It’s worth the work.
Puppy playdates are a part of socialization worth a special mention. They can turn early puppyhood from a challenge into a joy by offering an appropriate outlet for that mouthy play and helping to wear out our little furniture-shredding friends. Playdates also dramatically build a puppy’s doggy communication skills, which help a dog defuse potentially unsafe encounters later in life. So seek those playdates out – but do your homework because, unlike playdates with adult dogs, these friends aren’t yet fully vaccinated. If their owner isn’t being careful, they could expose your pup. So play only with pups who:
• have been in their homes (and away from a high-risk location like a shelter or puppy mill) for at least two weeks,
• are exhibiting absolutely no symptoms,
• are in the middle of their vaccination series with a vet,
• belong to an owner who is being careful about exposures.
As you work to make nuanced decisions about who your pup meets and where he goes, remember that you can stack the deck in your pup’s favor. “Good nutrition, regular deworming, flea and tick control, and good hygiene during this time are paramount in enabling a puppy to develop a healthy immune system,” says Dr. Hunt.
This COVID-19 is horrific – and yet it has increased the time people can spend with their dogs, resulted in soaring numbers of fostering and adoptions, lured many people into fostering, and increased many owners’ interest in dog training. I believe it will also help puppy owners practice the assessment skills so critical to disease risk management. Then more folks can confidently get their little puppies out and about, forming a lifelong impression that the world is full of new and wonderful things.

My young dog flies across the yard, tossing his ball in the air, chasing it as it hits the ground, then picks it up and tosses it again. I look over to see my toddler take off running in the opposite direction, giggling wildly. One arm is in the air, his fingers clutching a stuffed toy. The happiness level in this scene is reaching epic heights when the toy slips from his fingers and tumbles to the ground. The pup sees this, races over, and snatches it up.
I gasp in anticipation of howls of protest from my son. But, something else happens. Something fascinating and much quieter.
This small, 20-month-old human pauses, walks over to the ball the dog dropped, calls him, and holds it out to him. The dog drops the stuffed animal and takes the ball from his hand gently. The boy picks up his toy, and they both return to their previous play.
And, exhale.
This scene was not a lucky fluke. These two were demonstrating thoughtfully developed relationship skills, slowly cultivated and practiced over (and over) for many months. As their mutual caregiver, the work of creating a respectful, loving relationship between all members of my family, two-legged and four, was incredibly important to me, but I had little knowledge about and no experience with integrating kids and dogs.
In consultation with experts and by reviewing past issues of WDJ (see a partial list on page 11), I learned the best ways to get your resident dog or dogs ready for a baby, good management for safety and sanity, and considerations to keep in mind should you be crazy enough to want to add a puppy to your family when you have a young child. With this critical knowledge, I was then able to begin the work of building these relationships.
Hard, yes, but so worthwhile, especially in light of new research.
In a recent study published in Pediatric Research, scientists found, after adjusting for other factors, that children ages 3 to 5 from dog-owning families were 30% less likely to have conduct problems than children of the same age in families without pet dogs. They were also 40% less likely to have difficulty relating to peers, and 34% more likely to show empathy and concern for others.
These data suggest that having a dog and interacting with it, through play or family walks, may be an important mechanism for facilitating young children’s social-emotional development.
As many in the dog world are acutely aware, laying a great foundation for a puppy to enjoy successful future relationships with kids calls for mindful socialization of puppies with children and positive interactions between them during the pup’s key developmental windows (for more on this, see page 10). Still, life is dynamic and learning about the world is ongoing for dogs and humans alike.
Mosey, my Border Collie, was raised with and lovingly handled by children from birth. As he grew, I made a point to continue cultivating his respectful behavior with children. Early on, he became that dog who would see a stroller in the distance and start getting the serious waggles.
However, spending time with and around children occasionally is a quite different thing than living with them from infancy, full time.
From the moment my son could crawl, if there was a dog in view, he was moving at a shockingly fast pace in that direction, drawn to the dog as if by magnetism. The speed-crawling happened at the same time his fast fingers got very grabby (a tough phase for us all), which was a worrisome combination for the otherwise kid-loving dog. Mosey’s body language screamed: “This makes me nervous!”
I knew instantly that I needed to change this interaction or it could devolve into a negative experience for both of them. Managing the situation for the safety of both of them was easy enough, but I also recognized that positively guiding this interaction would provide an avenue to help them understand and respect one another.
I asked Celia Caldwell, a licensed clinical social worker in Missoula, Montana, who has worked for decades helping both foster children and dogs find and settle into loving homes, how I should best approach this. She advised, “You have to be a neutral Switzerland and hold safe space for both sides, allowing them to come together on their own terms.”
Caldwell stressed the importance of distance and making sure they both were able to express their curiosity about one another without pressuring or worrying the other.
In past articles in WDJ, Training Editor Pat Miller has advocated for the liberal use of baby gates (to secure those neutral lands), which my huband and I employed at any time when we couldn’t actively supervise the interactions between Mosey and our son Ansel. But, given an important bit of wisdom from Caldwell, we also strived to keep relations easy and fun between both of the knee-high parties.
“Remember that there is no bad behavior here, neither one is in the wrong,” advised Caldwell. “They simply need to learn how to understand one another and that takes time. Relationships take time and patience to develop.”
So, as just one tactic to keep them safe, separate, and unhassled, as soon as I’d see my son heading toward Mosey, I’d shout, “Incoming!” and grab Mosey’s beloved Frisbee. He’d race outside, and I’d throw the flying disc for him. A typical Border Collie, it took maybe two repetitions for him to learn this new cue.
We’d sometimes play another game when Mo flew back in with his Frisbee and stood holding it in front of me. I would pick up my son who would tap the Frisbee; this would make Mosey shake his head and wave the toy wildly, which would prompt equally wild giggles from my son. This became a daily shared joy.
When my son was 9 months old, I watched him peering out the window and, to my surprise, Mosey quietly sidled up to and leaned against him and he leaned back. They sat together contentedly watching the birds, and my heart exploded.
Getting to that moment was by no means instant, but they’ve been growing closer ever since, proving the tremendous value of patience.

Not all children are instinctually eager to jump into the canine fray, however. Just like with dogs, personalities and temperaments vary. Children with a cautious, slow-to-warm-up temperament prefer to investigate every situation carefully. These children learn through observation and may be more inclined to think through situations before they act, which can be a valuable instinct.
These children have as much potential to develop respectful, loving relationships with the four-legged members of your family as the dog-magnets, but will just require extra time and patience to get there. As their caretakers, it’s our job to pay attention and meet our child where they are and guide them through the world at their pace.
This is easier said than done. Sometimes – surprisingly often – we get in the way.
“What I stress with foster parents is the importance of leaving your ego out of it,” Caldwell told me. “You have to let the child decide how much is too much and when more is okay. And you won’t always do this perfectly. Expect to make mistakes.”
Well, I did. When we added a mixed-breed puppy to our family, we were thrilled to discover that Pip the pup loved our toddler as much as our toddler loved dogs. Pip is the ultimate Velcro dog, and he chose Ansel to be physically attached to – so cute! So sweet!
But even my dog-loving toddler had limits I needed to honor. Ansel began to express a weariness toward the amount of physical contact that Pip wanted to have with him, and I admit that I failed to see this right away. Had I kept Ansel’s complaints in my blind spot, I may have set their relationship back. It wasn’t until he wailed in utter frustration one day, as the pup plopped on him for the third time while he was assembling his trains, that I finally realized the error in my ways and created the space my son needed.
Again, I could easily manage this situation – pop the pup in a crate with a tasty treat! – but it presented a good opportunity to build the puppy’s skills and develop mutual respect.
I mat-trained Pip, setting the mat near wherever my son was playing, so when Pip got too close, I could ask him to go to his mat, where he would sit quietly. Months of practicing this lead to the day when I heard my son say, “Go to the mat” and looked up to see the pup go lie down, giving Ansel the space he needed. By no means did I expect a small child to play this role, but I was thrilled that he had learned through my excessive repetition to communicate respectfully and that the pup was happy to comply.
Through this ongoing work, I’ve gained a deeper understanding of the human-animal bond and the capacity of species to trust and genuinely care for one another.

• “Kids and Dogs,” August 2019. The formula for keeping children and canines safe is simple: Parents need to be attentive, assiduous about management, and quick to separate them at the first sign of the dog’s discomfort.
• “Dogs and Children: How to Keep Them Both Safe,” March 2018. Combining kids and dogs in your family can be magical and heartwarming, or cause a devastating tragedy. Here’s how to boost the odds of the former and prevent the latter.
• “The Puppy-Raising Challenge,” November 2017. Managing and training a young puppy can be exhausting, even for highly experienced dog trainers. Here are tips for taking some of the pressure off.
• “Teaching Kids to Love Dogs From an Early Age,” May 2012. How to raise kids who get along well with dogs and dogs who love kids in return.
• “Selecting the Best Family Dog and Preparing Him for Children,” August 2009. Protect everyone in your family (the dog, too) by selecting a good family dog and getting him ready for kids.
• “The relationship between dog ownership, dog play, family dog walking, and pre-schooler social-emotional development: Findings from the PLAYCE observational study,” Pediatric Research, July 6, 2020
• “Evidence of large genetic influences on dog ownership in the Swedish Twin Registry has implications for understanding domestication and health associations,” Scientific Reports, May 2019
• “Mat Training Tips,” Whole Dog Journal, January 2020. How a simple mat (and a little bit of training) can enhance your dog’s life – and yours, too!
Long-time WDJ contributor Kathryn Socie-Dunning lives in Montana with her husband, toddler son, and two snow-loving dogs.

Once upon a time, societal norms dictated that if pet dogs failed to comply with strict rules for their behavior indoors, they were banished to the outdoors. When I was a child, dog trainers of the day often told clients that allowing their dog on the bed or other furniture would give the dog too much privilege and let him think he could take over (dominate) the household.
Well, the times, they are a-changing.
These days, progressive, science-based, force-free training and behavior professionals recognize that most dogs are not trying to be dominant when on the couch; they are just trying to be comfortable – and perhaps want to be close to the humans they love!
You can use couch time as reinforcement for behaviors that you like (such as being friendly and cuddly) and temporarily revoke couch privileges for undesirable behaviors (such as being too pushy or insistent about climbing into your lap if you prefer your dog curl up quietly next to you). A cheerful, “Oops, off!” (with a treat tossed onto the floor if you haven’t yet taught the “Off” cue to your dog) will remove her from your lap, and a “Wait” cue will keep her on the floor until you are ready to invite her up. No dominance about it!
Also, the truth is, what you allow your dog to do in your own home is your choice – and while it may result in behaviors that others consider “bad manners,” that’s really up to you. In your house, you get to make the rules!
Here are some common rules from the past that many dogs (and their humans) now scoff at:
■ No dogs on the furniture. From 60 years ago to today, all the members of my family have allowed dogs on the furniture – and none of our dogs have ever staged a canine coup.
I love the solid feel of a warm dog’s body against my back in bed, and my evenings are generally spent on the sofa watching television and typing on my laptop, with our small dog Sunny snuggled up against my right side and medium/large Kai curled up on my left. I suspect Kai lived in a “No dogs on the furniture” household before he came to us; even after living with me and my husband for almost six years, I still have to reassure him that it’s okay to jump up on the sofa and often need to coax him up with a treat (although he jumps on the bed with no coaxing needed).
Of course, if you choose not to have dogs (and dog hair, drool, dirt, and leaves) on your furniture, that’s fine, too. But you are missing out on one of the greatest joys of sharing your home with a dog! We keep our furniture covered and whisk the covers off when company comes to reveal pristine furniture underneath.
Note: If allowing your dog on the furniture contributes to an inappropriate behavior such as growling as someone approaches, then you may need to restrict furniture access while you work to modify the behavior. See “Changing a Resource-Guarder,” WDJ May 2020, and “Resource-Guarding and What to Do About It,” August 2015, for more information about management and training protocols for this behavior.
■ No begging at meals. When I was a child, my mom often complained about my dad’s habit of feeding food scraps to our dogs from the table – but he did it anyway. This dynamic is intact in my home some 50-plus years later, as my husband Paul freely tosses bits of cheese, veggie sticks, popcorn, and whatever else he might be eating to our dogs. Sunny and Kai politely sit six or eight feet back from his chair, waiting in eager anticipation for the next tidbit.
While I freely share treats with my dogs throughout our days together, I choose to not feed them while I am eating my meals, and hence they never “beg” from me while I eat.
The good news: Dogs can learn to be attentive to one treat-dispensing family member and not bug others.
If you want to ensure your canine family members don’t get too pushy for treats but you’d still like to toss them a bit of your food from time to time, you can use mat training to teach them some impulse control along with their proximity to your table and the delicacies thereon. (See “Useful Matters,” January 2020.)

■ No jumping up. I used to be as adamant as anyone about teaching my dogs to greet people politely – and we still teach polite greetings in the Basic Good Manners classes taught at my training center. However, Sunny, our 25-pound Pomeranian/American Eskimo Dog-mix, has convinced us there can be value in having your dog jump up.
For one thing, Sunny is reasonably small and there’s generally no real harm done if he puts his paws up on you. For another, when he came to us, he was somewhat wary of new people, especially men (including Paul), and I didn’t want to discourage him from interacting with people in any way. Finally, he delights in leaping up in the air so I can catch him in my arms, and that’s just so darn cute I don’t have the heart to discourage the behavior. In fact, we show it off to friends.
You can still teach your dog to greet people politely but also teach her a “jump up” cue, making sure she gets reinforced for jumping up only if she’s asked to do so. This is especially helpful if one or more family members enjoy having the dog jump up on them. (For more about teaching a polite greeting, see “Meet and Greet? Or Not!” September 2018.)
■ Only go to the bathroom outdoors. Whaaat? Is there any other acceptable alternative to this?
Actually, there is! People who live in in highrise buildings sometimes find it to be near impossible to get their dogs outside in time; in this case, it makes sense to create a “legal” indoor canine bathroom.
This doesn’t mean the dog can go anywhere she wants in the apartment; there is still a designated place to eliminate. There is a variety of indoor litter boxes and types of absorbent substrate for dogs available in pet specialty stores and online. Some use litter, some use artificial grass, and some use real grass. Just Google “dog litter box” to find them.
■ No barking. It’s interesting to note how many of the old rules have to do with natural, normal canine behaviors. Sadly, far too many trainers today encourage their clients to use “no-bark” collars (shock or spray) to punish their dogs for barking, rather than allowing dogs to bark when it’s appropriate and teaching them to be quiet when it’s not. (See “Why Dogs Bark and How to Stop Them,” March 2017.)
We happen to have two dogs who are quite adept at barking, and both of them have high-pitched barks that can grate on your nerves. We’re fortunate that we live smack dab in the middle of our 80-acre farm; I can turn them out in the backyard and if they choose to bark at the horse in the pasture behind their fence, or wildlife in the woods, no one will complain.
When we are in the house, I do appreciate them barking to let me know that someone has pulled in the driveway (I can’t hear the cars drive in, but they can). However, the arousal/excitement barking when we head toward the door to go to the barn can get on my nerves. We’re working on that one.

Lest you get the impression that my dogs are unruly monsters who run amok in our home, let me assure you that is not the case. We do have rules, just not the same rules that were once commonplace in many dog homes:
■ Wait for the food bowl. Not only is this just a polite behavior and the easiest way to teach a “Wait” behavior, it’s also an excellent impulse-control exercise and keeps feeding-time chaos to a minimum.
The chaos part was more important for us in past years when we had five dogs, but it’s helpful even with our current two. Sunny and Kai each go to their feeding spots while I prepare their meals and offer a default sit as I approach them to feed. I cue them to “Wait,” place the bowl on the floor, mark with a “Yes,” feed a treat, and then say “Okay” and release them to eat. (See “Wait for the Food Bowl,” next page.)
■ Wait at the door. This life-saving rule applies at every door that goes to the outside world, as well as getting out of the car. It’s easy to teach and is great insurance against door-darting. Sunny and Kai have gotten so good at it we can even leave barn gates open while we’re feeding horses and they don’t go out unless invited. If you have already taught “Wait for the Food Bowl,” it’s a pretty simple matter to generalize it to doors and other places.
■ Wait at the top of the stairs.
I like this one because it allows me to make my way safely down the stairs without worrying about tripping over excited dogs. Again, it is simple to generalize this one quickly if your dog already knows “Wait” in a different application. Start at the top of the stairs, tell your dog to “Wait,” go down one step, mark, return and feed. Continue one step at a time until you’re all the way down, then invite your dog(s) to join you.
■ No wrestling in the house. There’s nothing wrong with allowing your dogs to roughhouse indoors if that’s what you want; I just prefer they do their wrestling outside. They play hard together in the barn and have learned that I will put them in the backyard if they wrestle indoors, so they now use it to let me know they want to – or have to – go outside. I love that they have taught me a cue!
■ No indoor arousal barking. Okay, true confession time: We are still working on this one.
It wasn’t a problem until Sunny arrived in our home two years ago, but he can be quite vocal, and when he starts, Kai happily joins in.
I judiciously use treats for “quiet” (positive reinforcement – dog’s behavior makes a good thing happen) and halt forward progress and turn my back when barking erupts (negative punishment – dog’s behavior makes a good thing go away). By using these complementary tactics, I can now make it down the stairs and out the back door on the way to the barn at 6 in the morning without a cacophony of barking. I’m sure when this pandemic is over and we once again have house guests, they will appreciate that.
Other than those, we of course have the normal, obvious house rules – no chewing on things you’re not supposed to chew on, no getting up on the counters, no chasing the cats, no getting in the garbage, etc. But overall, having fewer rules and allowing your dog to make more of her own choices in your home makes for a behaviorally healthier companion and a better relationship between the two of you. So yes, have the rules that you need and want, but don’t let anyone else tell you what they should be. It’s your house; you get to make the rules.
What do I most appreciate about the “Wait” behavior? It’s easy for dogs to learn and easy for them to generalize “Wait!” to a variety of situations in which you want them to pause where they are for a few moments, until given a cue to proceed.
Here’s how to teach this highly useful behavior:
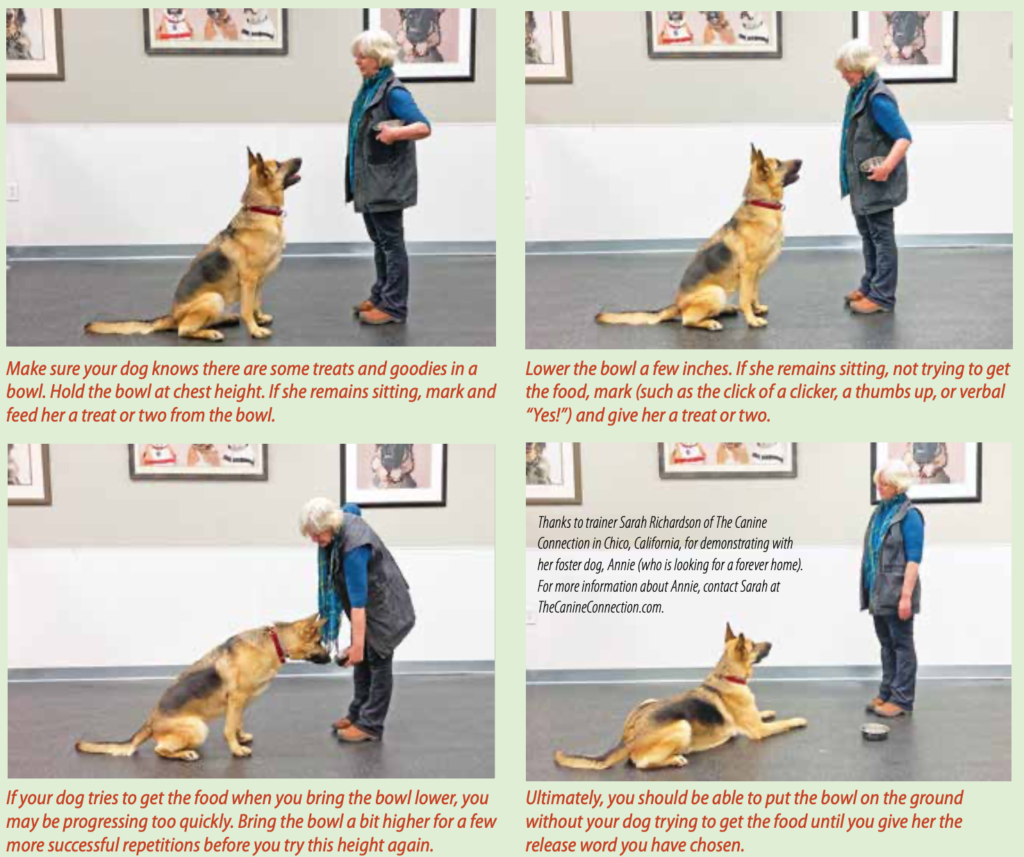
1. With your dog sitting, facing you, hold her bowl at chest level (with food in it, topped with tasty treats) and say “Wait.”
2. Lower the food bowl toward the floor two inches. If your dog remains sitting, click your clicker (or use a verbal marker, such as the word “Yes!”), raise the bowl back up again, and feed her a treat from the bowl. If she gets up, say “Oops” and ask her to sit again. If she remains in place, lower the bowl two inches again, mark (click or “Yes!”), raise the bowl, and treat.
3. Repeat this step several times until she remains sitting as you lower the bowl. Mark and treat each time.
4. Gradually move the bowl closer to the floor with succeeding repetitions until you can place it on the floor two feet away from her and pick it back up without her getting up or trying to eat it.
5. Finally, place the bowl on the floor and say a release cue to tell her to eat. Note: Choose your release cue carefully. Many people use “Okay!” as their release cue, but a common word like this may accidentally release your dog when you are casually speaking to someone as the dog waits. Consider alternatives such as “Free!” or “Done!”
A really helpful thing about teaching this behavior is that you have at least one built-in daily practice session (possibly two, since many of us feed our dogs twice a day). To teach other Wait applications, break the behavior down to small steps: Wait while you reach for the door. Wait while you jiggle the doorknob. Wait while you open the door a crack. Wait while you open it a little farther. And so on.

Have you ever bought a cute but pricey item in a pet supply store, only to have it fail within days – or hours? “Super tough” toys that don’t make it through a day of play, beds with zippers that permanently separate the first time you wash the cover, collars that cost an arm and a leg but fray or fade within a short time I think we’ve all been there. Well, in brief: This stuff ain’t that! Here are some of the most worth-it dog-related items we’ve tried this year.
 It’s normal to have one dog and 17 stuffable food puzzles, right? Normal or not, my dog fully supports my obsession, and we were both excited to add the Toppl to our line-up. The Toppl is a cup-shaped toy with a rounded bottom, and extending from the bottom of the inside of the cup, five long, flexible inner fingers (they call them “teeth”) that hold treats in place. The easiest extraction project for dogs who are inexperienced with food-dispensing toys is to insert treats between the inner teeth. For an added challenge, a small and large Toppl can be connected to each other with kibble or other small treats inside. Since each Toppl has a rounded hole on its side, the kibble will dribble out as a dog manipulates and rolls the conjoined toys around.
It’s normal to have one dog and 17 stuffable food puzzles, right? Normal or not, my dog fully supports my obsession, and we were both excited to add the Toppl to our line-up. The Toppl is a cup-shaped toy with a rounded bottom, and extending from the bottom of the inside of the cup, five long, flexible inner fingers (they call them “teeth”) that hold treats in place. The easiest extraction project for dogs who are inexperienced with food-dispensing toys is to insert treats between the inner teeth. For an added challenge, a small and large Toppl can be connected to each other with kibble or other small treats inside. Since each Toppl has a rounded hole on its side, the kibble will dribble out as a dog manipulates and rolls the conjoined toys around.  But to me, where the Toppl truly shines is its ease of use when it comes to stuffing and freezing a portion of a dog’s meal. I’m a longtime Kong user and routinely mix kibble with any number of “binders” (yogurt, canned pumpkin, mashed sardines, diluted peanut butter) and stuff the concoction into Kongs. It takes a little work to squeeze the goopy mix into the one-inch opening of even the largest Kong toys. In contrast, the opening on a large Toppl is two inches, and even the small Toppl’s opening is a user-friendly 1 ¾ inches. This makes them much easier to quickly stuff – a fact I greatly appreciate late on a Sunday night when I’m getting ready for a busy workweek.
But to me, where the Toppl truly shines is its ease of use when it comes to stuffing and freezing a portion of a dog’s meal. I’m a longtime Kong user and routinely mix kibble with any number of “binders” (yogurt, canned pumpkin, mashed sardines, diluted peanut butter) and stuff the concoction into Kongs. It takes a little work to squeeze the goopy mix into the one-inch opening of even the largest Kong toys. In contrast, the opening on a large Toppl is two inches, and even the small Toppl’s opening is a user-friendly 1 ¾ inches. This makes them much easier to quickly stuff – a fact I greatly appreciate late on a Sunday night when I’m getting ready for a busy workweek.  The rubbery Toppl comes in two sizes (large is four inches tall; small is three inches) and three colors (blue, orange, and green). The Toppl is top-rack dishwasher safe, latex-free, and FDA-compliant (safe to eat from). All West Paw products are made in the USA. The proprietary plastic blend is recyclable; you can’t toss your worn out toys into your own recycling bin, but you can send them back to West Paw’s Bozeman, Montana, facility and they’ll recycle them into new dog toys! The company also offers a “Love It Guarantee,” which entitles customers to a one-time refund or replacement per toy design. – Stephanie Colman
The rubbery Toppl comes in two sizes (large is four inches tall; small is three inches) and three colors (blue, orange, and green). The Toppl is top-rack dishwasher safe, latex-free, and FDA-compliant (safe to eat from). All West Paw products are made in the USA. The proprietary plastic blend is recyclable; you can’t toss your worn out toys into your own recycling bin, but you can send them back to West Paw’s Bozeman, Montana, facility and they’ll recycle them into new dog toys! The company also offers a “Love It Guarantee,” which entitles customers to a one-time refund or replacement per toy design. – Stephanie Colman
 I was given a prepublication copy of this book and asked if I would consider writing a blurb for its promotion. “Would I? Would I?” I took the additional step of immediately asking its author if she’d start writing for WDJ, and her articles (including the one on page 15 of this issue) have been a bright light in a dark year.
I was given a prepublication copy of this book and asked if I would consider writing a blurb for its promotion. “Would I? Would I?” I took the additional step of immediately asking its author if she’d start writing for WDJ, and her articles (including the one on page 15 of this issue) have been a bright light in a dark year.  In 101 Rescue Puppies, dog trainer and serial foster provider Kathy Callahan tells warm, funny, and heart-rending stories about fostering litters of puppies for shelters and rescues in her area. Callahan relates how foster providers can reverse the arc of homeless animal stories, transforming tragic origin tales into supremely happy endings, just by giving pups some time in a clean space with loving attention, nourishing food, a good bit of cleanup, and social connections to good-hearted, responsible adopters. I guarantee that her warm portraits of the pups, in words and pictures, will make every reader laugh and cry several times – and, I hope, encourage at least a few to try providing foster care for needy animals themselves. – Nancy Kerns
In 101 Rescue Puppies, dog trainer and serial foster provider Kathy Callahan tells warm, funny, and heart-rending stories about fostering litters of puppies for shelters and rescues in her area. Callahan relates how foster providers can reverse the arc of homeless animal stories, transforming tragic origin tales into supremely happy endings, just by giving pups some time in a clean space with loving attention, nourishing food, a good bit of cleanup, and social connections to good-hearted, responsible adopters. I guarantee that her warm portraits of the pups, in words and pictures, will make every reader laugh and cry several times – and, I hope, encourage at least a few to try providing foster care for needy animals themselves. – Nancy Kerns
 This is a 100% true story; I swear on my dogs’ health:
This is a 100% true story; I swear on my dogs’ health:  Already a fan of these collars just based on their principle and design, I was photographing one that had been sent to me before trying it out on my own dogs; once one of my dogs had worn it for a while, it was never going to look clean and new again. I took pictures of the collar on a table and then put it on my little foster dog Coco to take pictures of it on her. Just then, my phone rang and I took the call; it was my sister. As I talked, Coco ran off to play with Woody, and they immediately began wrestling and playing the kind of bitey-face games they enjoy – and the kind of games that this collar was invented for: to prevent accidental strangulation. As their game escalated, I told my sister I had to go and I started taking pictures of Woody and Coco’s rough play.
Already a fan of these collars just based on their principle and design, I was photographing one that had been sent to me before trying it out on my own dogs; once one of my dogs had worn it for a while, it was never going to look clean and new again. I took pictures of the collar on a table and then put it on my little foster dog Coco to take pictures of it on her. Just then, my phone rang and I took the call; it was my sister. As I talked, Coco ran off to play with Woody, and they immediately began wrestling and playing the kind of bitey-face games they enjoy – and the kind of games that this collar was invented for: to prevent accidental strangulation. As their game escalated, I told my sister I had to go and I started taking pictures of Woody and Coco’s rough play.  Just then, as is his habit, Woody grabbed onto Coco’s collar; he likes to drag other dogs around by any gear they happen to be wearing. Coco squirmed to get away and as she did, she wildly rolled over, and for a single second, Woody’s mouth was stuck on her collar. And then, nearly instantaneously – POP! The collar’s safety mechanism did what it was designed to do and the collar snapped apart, freeing Coco.
Just then, as is his habit, Woody grabbed onto Coco’s collar; he likes to drag other dogs around by any gear they happen to be wearing. Coco squirmed to get away and as she did, she wildly rolled over, and for a single second, Woody’s mouth was stuck on her collar. And then, nearly instantaneously – POP! The collar’s safety mechanism did what it was designed to do and the collar snapped apart, freeing Coco.  For just a moment, Woody stood with the collar in his mouth, looking confused; that had never happened to him before! And Coco jumped to her feet and scampered away – both dogs unharmed. It was a perfect demonstration of how dangerous a conventional collar would have been, and how perfectly this collar performs to eliminate the threat that normal collars pose to dogs who play this sort of game. I can’t believe I was standing right there taking pictures when it happened.
For just a moment, Woody stood with the collar in his mouth, looking confused; that had never happened to him before! And Coco jumped to her feet and scampered away – both dogs unharmed. It was a perfect demonstration of how dangerous a conventional collar would have been, and how perfectly this collar performs to eliminate the threat that normal collars pose to dogs who play this sort of game. I can’t believe I was standing right there taking pictures when it happened.  In the December issue, I wrote an article (“Don’t Wait! Prevent Collar Accidents”) about the strangulation dangers that regular collars can pose to dogs, and I mentioned a product that was designed to eliminate these dangers. As it turns out, I described an early prototype of the current collar, one that’s no longer made. The collar whose effectiveness Woody and Coco just demonstrated is the new and improved model of the product I described. The owners of Chinook & Co., LLC, invented this collar after their dog Chinook died in a collar strangulation accident. The collar features standard plastic side-squeeze buckles, a tiny loop for attaching an ID tag, and a sizing adjustment slider. But the big draw of the collar is its patented break-away buckle, which releases automatically when pressure is applied. The buckle can be re-fastened quickly and easily. Of course, no one wants their dog’s collar to release when they are walking their dog or to have to change collars every time they are about to go for a walk. So the KeepSafe collar has two leash-attachment D-rings; you snap your leash to both of them to override the breakaway feature. Chinook & Co. has a relationship with PetSafe, who sells the red, blue, and black KeepSafe Break-Away collars on their website. But the inventors offer an exclusive line of the collars in nine colors and patterns that they sell directly from their website: breakawaycollar.com. – N.K.
In the December issue, I wrote an article (“Don’t Wait! Prevent Collar Accidents”) about the strangulation dangers that regular collars can pose to dogs, and I mentioned a product that was designed to eliminate these dangers. As it turns out, I described an early prototype of the current collar, one that’s no longer made. The collar whose effectiveness Woody and Coco just demonstrated is the new and improved model of the product I described. The owners of Chinook & Co., LLC, invented this collar after their dog Chinook died in a collar strangulation accident. The collar features standard plastic side-squeeze buckles, a tiny loop for attaching an ID tag, and a sizing adjustment slider. But the big draw of the collar is its patented break-away buckle, which releases automatically when pressure is applied. The buckle can be re-fastened quickly and easily. Of course, no one wants their dog’s collar to release when they are walking their dog or to have to change collars every time they are about to go for a walk. So the KeepSafe collar has two leash-attachment D-rings; you snap your leash to both of them to override the breakaway feature. Chinook & Co. has a relationship with PetSafe, who sells the red, blue, and black KeepSafe Break-Away collars on their website. But the inventors offer an exclusive line of the collars in nine colors and patterns that they sell directly from their website: breakawaycollar.com. – N.K. 
 We love freeze-dried meats for use in dog diets and especially for treats. Freeze-drying preserves the meaty aroma of the main ingredients, but the treats are non-greasy and so low in moisture that they have a long shelf life, even after a package is opened. For a long time, our hearts belonged solely to Stella and Chewy’s, who innovated a certain type of puffy nugget of freeze-dried meat. We still love that company’s Meal Mixers, but we have opened our hearts and wallets to Rawbble, a very similar product offered by Bixbi Pet. Why? Well, for one, Rawbble’s nuggets are smaller in size, making it more appropriate for feeding in a training session with small or tiny dogs. (The nuggets are easily squished between the fingers to divide them into still smaller treats, but when working with a dog at a fast pace, it’s just easier to dole out the nuggets in their original form.)
We love freeze-dried meats for use in dog diets and especially for treats. Freeze-drying preserves the meaty aroma of the main ingredients, but the treats are non-greasy and so low in moisture that they have a long shelf life, even after a package is opened. For a long time, our hearts belonged solely to Stella and Chewy’s, who innovated a certain type of puffy nugget of freeze-dried meat. We still love that company’s Meal Mixers, but we have opened our hearts and wallets to Rawbble, a very similar product offered by Bixbi Pet. Why? Well, for one, Rawbble’s nuggets are smaller in size, making it more appropriate for feeding in a training session with small or tiny dogs. (The nuggets are easily squished between the fingers to divide them into still smaller treats, but when working with a dog at a fast pace, it’s just easier to dole out the nuggets in their original form.)  Both Stella and Chewy’s Meal Mixers and Bixbi Pet’s Rawbble are nutritionally complete and balanced for dogs of all life stages and could be fed as a sole diet. However, Rawbble’s formulas contain fewer ingredients; the animal protein ingredients are a higher percentage of the food. And even so, they cost a little less than their competitor’s products. Rawbble is available in six single-species formulas (beef, chicken, duck, lamb, pork, and turkey) and one formula with two species (chicken and salmon). Each contains muscle meat (with ground bone) as well as specified organ meat (liver, kidney, and/or heart of the same species as the muscle meat). All of the products are USA-sourced and -made. Buy a small bag (4.5 ounces, for $10 to $12, depending on the formula), offer it to your dog in a training session, and we guarantee you’ll soon find yourself buying the more economical large bags (26 ounces, for $48 to $57, depending on formula). – N.K.
Both Stella and Chewy’s Meal Mixers and Bixbi Pet’s Rawbble are nutritionally complete and balanced for dogs of all life stages and could be fed as a sole diet. However, Rawbble’s formulas contain fewer ingredients; the animal protein ingredients are a higher percentage of the food. And even so, they cost a little less than their competitor’s products. Rawbble is available in six single-species formulas (beef, chicken, duck, lamb, pork, and turkey) and one formula with two species (chicken and salmon). Each contains muscle meat (with ground bone) as well as specified organ meat (liver, kidney, and/or heart of the same species as the muscle meat). All of the products are USA-sourced and -made. Buy a small bag (4.5 ounces, for $10 to $12, depending on the formula), offer it to your dog in a training session, and we guarantee you’ll soon find yourself buying the more economical large bags (26 ounces, for $48 to $57, depending on formula). – N.K.
 This little hard-backed book, just six inches tall, packs more information about canine body language into 126 pages than hours of video narrated by a canine behavior expert. Author and illustrator Lili Chin is a supremely talented artist, and the dogs she draws are adorable. But she also happens to be gifted with the ability to reproduce the immediately recognizable expressions and postures of dogs in responding to things and events with fear, excitement, anxiety, happiness, stress, and calm acceptance.
This little hard-backed book, just six inches tall, packs more information about canine body language into 126 pages than hours of video narrated by a canine behavior expert. Author and illustrator Lili Chin is a supremely talented artist, and the dogs she draws are adorable. But she also happens to be gifted with the ability to reproduce the immediately recognizable expressions and postures of dogs in responding to things and events with fear, excitement, anxiety, happiness, stress, and calm acceptance. 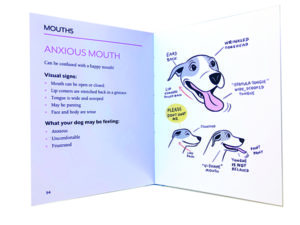 But while most dog owners will recognize the body language that Chin illustrates, many are unable to interpret what they are seeing, and thus will misunderstand what their dogs may be trying to tell them. So Chin breaks it down and explains, in chapters devoted to the particular language of canine greetings, conflict, stress, and play, with special focus on the variations in what dogs “say” with their eyes, posture, mouths, ears, and tails.
But while most dog owners will recognize the body language that Chin illustrates, many are unable to interpret what they are seeing, and thus will misunderstand what their dogs may be trying to tell them. So Chin breaks it down and explains, in chapters devoted to the particular language of canine greetings, conflict, stress, and play, with special focus on the variations in what dogs “say” with their eyes, posture, mouths, ears, and tails.  Chin sells her art and products online and is in demand as a creator of educational materials for veterinarians, dog behavior consultants, and dog training organizations – and no wonder! Her enaging illustrations and brief, clear descriptions make it possible for anyone to understand what dogs are telling us (and each other). This would be an equally appropriate book to give a dog-crazy child, an adult who was adopting a dog for the first time, or a long-time dog owner who has been having trouble understanding her dog. – N.K.
Chin sells her art and products online and is in demand as a creator of educational materials for veterinarians, dog behavior consultants, and dog training organizations – and no wonder! Her enaging illustrations and brief, clear descriptions make it possible for anyone to understand what dogs are telling us (and each other). This would be an equally appropriate book to give a dog-crazy child, an adult who was adopting a dog for the first time, or a long-time dog owner who has been having trouble understanding her dog. – N.K.
 There’s probably not one of us who hasn’t spent a lot of money on dog beds throughout the years of living with one or multiple dogs– too frequently, in my case! Often, the chosen product didn’t quite live up to my standards for quality or ease of cleaning – or my dogs’ comfort!
There’s probably not one of us who hasn’t spent a lot of money on dog beds throughout the years of living with one or multiple dogs– too frequently, in my case! Often, the chosen product didn’t quite live up to my standards for quality or ease of cleaning – or my dogs’ comfort!

Sound familiar? Thankfully, your faith in a high-quality, comfy, easy-to-clean bed can be restored with the Wash ‘n Zip Pet Bed. Imagine a nice, large quilted blanket, folded in half, then folded in half again; then imagine zipping a zipper that goes around the three sides of the folded blanket, holding the blanket into a nice, thick rectangle. That’s the Wash ‘n Zip! (Note that the smaller sizes are folded over only once, not twice.) Of the many things I love about this bed, the convenience of washing it is tops. The entire bed can easily be unzipped and put in the washer and dryer; there’s no wrestling with removing and replacing a cover. I cannot tell you how amazed I am each and every time with how easily the bed zips back together after washing and drying. I’ve also used the unzipped bed as a car seat or couch cover and as a blanket for a picnic with my dogs!  The Wash ‘n Zip is constructed of rugged materials with quality stitching and a heavy-duty zipper. The materials of the bed are nontoxic, and the sheets of interior batting are box-stitched to lock the batting in place so that the bed holds its shape over time. The beds come in five different sizes, with the smallest being 24 x 18 inches (zipped) and the largest 48 x 34 (zipped). There are four color choices, with three of them available in a soft velour fabric and the fourth in a soft fleece; the underside of all the beds is made of a khaki-colored, strong poly/cotton material. Even before the pet bed arrived, I was blown away by the superior customer service of this independently owned small business. With a new puppy in our home, I needed a brand new bed. My order barely had time to process before the owner of the company emailed me back, apologizing that he was currently out of my chosen color. He asked if I’d be okay with his shipping me a similar color tone fabric to use while the other was on back order. I agreed and let him know I’d be using the bed for our new puppy. With that news, the high level of customer service only increased; the owner threw in a Puppy Proofer, a cover that fits over the bed and closes with Velcro on the bottom, helping to prevent damage from the shark-like teeth of a puppy’s chewing habits (or even an adult dog who is a prolific chewer). Wow! When the products arrived, we found that the cover was easy to put on and take off, and helps keep the bed cleaner, for less-frequent washing. The bed is cushy enough for our arthritic senior dog, who spends his most of his days lazing around, but not so deep that he has difficulty rising. But if the bed didn’t provide quite enough padding for your dog, the company also sells an additional “comfort cushion” that’s made to fit inside the beds. The cushion is a one-piece, box-stitched washer/dryer friendly insert.
The Wash ‘n Zip is constructed of rugged materials with quality stitching and a heavy-duty zipper. The materials of the bed are nontoxic, and the sheets of interior batting are box-stitched to lock the batting in place so that the bed holds its shape over time. The beds come in five different sizes, with the smallest being 24 x 18 inches (zipped) and the largest 48 x 34 (zipped). There are four color choices, with three of them available in a soft velour fabric and the fourth in a soft fleece; the underside of all the beds is made of a khaki-colored, strong poly/cotton material. Even before the pet bed arrived, I was blown away by the superior customer service of this independently owned small business. With a new puppy in our home, I needed a brand new bed. My order barely had time to process before the owner of the company emailed me back, apologizing that he was currently out of my chosen color. He asked if I’d be okay with his shipping me a similar color tone fabric to use while the other was on back order. I agreed and let him know I’d be using the bed for our new puppy. With that news, the high level of customer service only increased; the owner threw in a Puppy Proofer, a cover that fits over the bed and closes with Velcro on the bottom, helping to prevent damage from the shark-like teeth of a puppy’s chewing habits (or even an adult dog who is a prolific chewer). Wow! When the products arrived, we found that the cover was easy to put on and take off, and helps keep the bed cleaner, for less-frequent washing. The bed is cushy enough for our arthritic senior dog, who spends his most of his days lazing around, but not so deep that he has difficulty rising. But if the bed didn’t provide quite enough padding for your dog, the company also sells an additional “comfort cushion” that’s made to fit inside the beds. The cushion is a one-piece, box-stitched washer/dryer friendly insert.  It’s been 2 1/2 years since I ordered my first Wash n’ Zip pet bed. I currently have three and am about to order a fourth. We have two dogs, but I want yet another bed! The price point, convenience of cleaning, and the versatility of the product makes it an easy decision to buy multiple beds in order to provide a soft spot in other rooms for our dogs. Did I mention that they travel well, too? I take one with me to our Fear-Free vet’s office to use atop their own soft matting. If you’re looking for a long-lasting, easy-to-clean bed that your dog will love, this is it. – Lisa Lyle Waggoner The Wash ‘n Zip bed, zipped all the way open. This size gets folded twice, making the bed four layers thick when it’s zipped up again. Lisa’s youngest dog, Cailie, enjoying her new bed.
It’s been 2 1/2 years since I ordered my first Wash n’ Zip pet bed. I currently have three and am about to order a fourth. We have two dogs, but I want yet another bed! The price point, convenience of cleaning, and the versatility of the product makes it an easy decision to buy multiple beds in order to provide a soft spot in other rooms for our dogs. Did I mention that they travel well, too? I take one with me to our Fear-Free vet’s office to use atop their own soft matting. If you’re looking for a long-lasting, easy-to-clean bed that your dog will love, this is it. – Lisa Lyle Waggoner The Wash ‘n Zip bed, zipped all the way open. This size gets folded twice, making the bed four layers thick when it’s zipped up again. Lisa’s youngest dog, Cailie, enjoying her new bed.
 Denise Fenzi, the author of Conversations with Raika, is a professional dog trainer and the owner/founder of Fenzi Dog Sports Academy, a highly successful online school for both competition and pet dogs. Fenzi has written a number of excellent books on training – but this isn’t one of them. Instead, it’s a series of imagined discussions that Fenzi had with her retired Obedience Champion Belgian Tervuren, Raika. The book’s introduction explains the “conversation” this way: “For a long while, Raika talked, but no one heard. She was not discouraged; her many years as a competition dog had taught her to persist in the face of challenge, so she just kept right on talking. And when that voice emerged, it was not nearly as agreeable nor lacking in opinions as one might have thought. Indeed, once she got started, Raika had opinions on everything from what time she went for her walk to what showed up in her food bowl to how she wanted to leave this earth, with plenty of commentary in between.”
Denise Fenzi, the author of Conversations with Raika, is a professional dog trainer and the owner/founder of Fenzi Dog Sports Academy, a highly successful online school for both competition and pet dogs. Fenzi has written a number of excellent books on training – but this isn’t one of them. Instead, it’s a series of imagined discussions that Fenzi had with her retired Obedience Champion Belgian Tervuren, Raika. The book’s introduction explains the “conversation” this way: “For a long while, Raika talked, but no one heard. She was not discouraged; her many years as a competition dog had taught her to persist in the face of challenge, so she just kept right on talking. And when that voice emerged, it was not nearly as agreeable nor lacking in opinions as one might have thought. Indeed, once she got started, Raika had opinions on everything from what time she went for her walk to what showed up in her food bowl to how she wanted to leave this earth, with plenty of commentary in between.”  A “talking dog” device in fiction can get cloying or annoying – but Fenzi channels the personality of her smart, challenging, opinionated, and insightful senior dog so skillfully that the reader “buys into” the conversation completely within just a few pages. This has just as much to do with the witty and humorous banter between the two long-time friends as the insights about life and death they share (or argue about) as they navigate Raika’s senior years to a moving conclusion. – N.K.
A “talking dog” device in fiction can get cloying or annoying – but Fenzi channels the personality of her smart, challenging, opinionated, and insightful senior dog so skillfully that the reader “buys into” the conversation completely within just a few pages. This has just as much to do with the witty and humorous banter between the two long-time friends as the insights about life and death they share (or argue about) as they navigate Raika’s senior years to a moving conclusion. – N.K.
 I’m pretty sure I can hear the gasps from here: HUNDREDS of dollars for a dog bed? How can any dog bed be worth that much? First, these are not just any dog beds. And they are beds that not many dogs may need. These are big dog beds for big dogs – big dogs, up to 250 pounds, who need extra-thick padding between their big bodies and big bones and the hard floor. Big Barker beds are made with three bonded layers of American-made foam with an astounding 10-year warranty. Yes, Big Barker guarantees that these beds will not flatten within 10 years, or you get a new bed. Also, Big Barker would like to warn dog owners about Chinese-made foam mattresses, which have been known to emit noxious odors and have tested positive for lead, arsenic, chlorine, and other potentially dangerous chemicals. Even the glue that’s used to bond the layers of foam together has been carefully sourced by Big Barker. They use an American-made water-based latex glue, which is fully OSHA-compliant and can be sprayed without masks or filtration.
I’m pretty sure I can hear the gasps from here: HUNDREDS of dollars for a dog bed? How can any dog bed be worth that much? First, these are not just any dog beds. And they are beds that not many dogs may need. These are big dog beds for big dogs – big dogs, up to 250 pounds, who need extra-thick padding between their big bodies and big bones and the hard floor. Big Barker beds are made with three bonded layers of American-made foam with an astounding 10-year warranty. Yes, Big Barker guarantees that these beds will not flatten within 10 years, or you get a new bed. Also, Big Barker would like to warn dog owners about Chinese-made foam mattresses, which have been known to emit noxious odors and have tested positive for lead, arsenic, chlorine, and other potentially dangerous chemicals. Even the glue that’s used to bond the layers of foam together has been carefully sourced by Big Barker. They use an American-made water-based latex glue, which is fully OSHA-compliant and can be sprayed without masks or filtration.  The material used for the Big Barker’s covers was chosen for its softness and durability. The company says their fabrics hold up well against digging and nesting. “Our strong microfiber covers score 100,000 or higher on the standard Wyzenbeek Abrasion test, which measures a fabric’s ability to withstand surface wear from rubbing. High-quality household furniture only requires scores of 15,000.” Only super-strong, American-made zippers are used for the covers. “Because our foam is so big and thick, we use up to 150 inches of zipper, surrounding a full 75% of the bed.” This enables you to take the cover off and put it back on after laundering with ease. The Big Barker bed is available in three sizes (the smallest is 30 x 48 inches; the largest is 48 x 60 inches) and two styles: flat (“Sleek Edition”) and with a headrest at one end (“Headrest Edition”). The covers are available in four solid colors. Like I said, not everyone will need these beds. But if you have a big dog – and particularly a big, old dog, you probably need one of these beds. At 70 pounds, my 13-year-old arthritic dog absolutely qualifies, and approves of this review. – N.K.
The material used for the Big Barker’s covers was chosen for its softness and durability. The company says their fabrics hold up well against digging and nesting. “Our strong microfiber covers score 100,000 or higher on the standard Wyzenbeek Abrasion test, which measures a fabric’s ability to withstand surface wear from rubbing. High-quality household furniture only requires scores of 15,000.” Only super-strong, American-made zippers are used for the covers. “Because our foam is so big and thick, we use up to 150 inches of zipper, surrounding a full 75% of the bed.” This enables you to take the cover off and put it back on after laundering with ease. The Big Barker bed is available in three sizes (the smallest is 30 x 48 inches; the largest is 48 x 60 inches) and two styles: flat (“Sleek Edition”) and with a headrest at one end (“Headrest Edition”). The covers are available in four solid colors. Like I said, not everyone will need these beds. But if you have a big dog – and particularly a big, old dog, you probably need one of these beds. At 70 pounds, my 13-year-old arthritic dog absolutely qualifies, and approves of this review. – N.K.

This is the first issue of WDJ’s 24th year of publication – wow! The only time that it genuinely feels like it’s been that long is when I sit down to write yet another editorial. I’ve written something to appear in this space every month for every one of WDJ’s 23 years!
These editor’s notes notwithstanding, the time has flown by – partially because so much in the dog world has changed in the past two-plus decades. In the early days of this publication, if a dog owner was looking for help training a puppy, he’d likely be told to bring his dog back after six (or more) months; puppy training wasn’t commonly available as the prevailing wisdom was that a dog had to be mature to handle training. Today we know that failing to start training during those first six months of a dog’s life is a colossal wasted opportunity, but it was probably just as well that people didn’t enroll puppies in training classes back then, because most dog-training facilities offered only “obedience” classes, and choke chains were mandatory equipment.
In 1998, Pat Miller was an early adopter of the newest training technologies, which were variously called positive-only, force-free, or dog-friendly. An experienced equestrian, Pat had been a regular contributor to another magazine published by Belvoir Media Group, The Whole Horse Journal (which, sadly, is no longer published). But she also was a dog trainer, and when she learned that Belvoir was launching a canine publication, she jumped at the chance to write for Whole Dog Journal. She had an article in WDJ’s first issue – and at least one article in every issue since, save one. (Sometime in WDJ’s first decade I once cut her article for lack of space and I don’t think she’s forgiven me for that yet!)
In the space of 23 years, compulsion-free dog training and puppy classes have evolved from a novelty scorned by the majority of professional trainers to the mainstream. Today, trainers who routinely use yanks on a choke chain to teach basic behaviors like sit and walking on a loose leash are the minority. I’d like to think that Pat’s articles, her relentless advocacy for the kind treatment of dogs and their handlers, and her recruitment of other force-free trainers to write for WDJ helped foment this gentle dog-training revolution.
Pat’s early fascination and aptitude with the most modern training theories and her dedication to the kindest, most compassionate, and most effective training techniques amply qualified her to lead WDJ in this area. It didn’t take long for me to recognize her leadership in the form of the “Training Editor” title. When it comes to behavior and training, she’s our lodestar, and I’m grateful to her for many years of patient tutelage and guidance.

The other day, I was working away on my computer, both dogs snoozing in my office while my Spotify playlist blared from the computer speakers. Suddenly, the music cut out – an interruption in my rural internet service or something – and it’s a good thing it did, for in those few moments of silence, I heard something that stops most of us dog owners in our tracks: the unmistakable sound of a dog’s repetitive licking that signals trouble.
“Hey!” I exclaimed, jumping up from my computer chair to see which dog was licking, and where. I clearly woke up Woody – it wasn’t him. But Otto, who had been laying in a door-less crate in my office, hung his head with a “Shoot! Caught in the act!” look. I asked him to come out of his crate for a quick exam.
He stepped out and the problem was immediately apparent: He had been licking a big raw spot on his hip – a spot that had not been there earlier in the day.

I asked Otto to lay down in the middle of my office floor and checked his tummy for fleas. In my experience, if a dog has fleas, you will see them running across the hairless or sparsely haired tummy first. On Otto: Nothing. I grabbed a flea comb and started combing. Flea combs have tiny teeth, packed very close together. You can work quickly to examine a thin-coated dog with one. But scruffy Otto has a fine undercoat, and flea combs pull a lot of loose hair out. I had to examine each comb-full of hair closely – I had to get my reading glasses to do so! – to make sure I spotted any flea or “flea dirt” (flea feces).
After about 20 minutes of combing, I found a single flea. Oh my lord, Otto.

My “heart dog” of yore, Rupert the Border Collie, had been severely allergic to flea bites, and if he was ever bitten by one, this is exactly what would happen: Within hours, he’d transform from a “regular” dog to anxious, neurotic, obsessed, and compulsive. He’d go crazy with scratching and chewing himself, as I raced to get him whatever was needed to stop his itching: something to nuke the fleas, something to stop the itching, something to calm him down.
Otto has not, for most of his life, been that sensitive. Since I foster fairly frequently, we’ve had the occasional flea incursion that had to be put down quickly. In instances of a transient flea invasion, Otto would get only mildly itchy. He’s never been covered with fleas, but, once or twice, we’d had a mild population boom. (I used to have a couch on a covered porch and the dogs liked laying on it. So did a neighborhood cat. Boom – all of a sudden, the couch was a flea farm. It went to the dump shortly afterward.) At 13 years old, though, Otto’s immune system seems to be twitchy.
Using an old pair of horse’s ear clippers I have, I clipped the hair surrounding the hotspot; when the hair touches skin that’s abraded and open, it constantly introduces bacteria to the site. Shaving the surrounding hair makes it look awful, but heal more quickly.

Next, I gently cleaned the site with a mild liquid antibacterial soap, and rinsed it well. Next, I dried the area all around with a clean towel, and used a hair dryer on “cool” to dry the hotspot itself. Finally, I used a favorite remedy, EMT Gel, to lightly coat the wound. We discussed this gel in an October 2013 article, “Alternative Treatment and Supplement Recommendations,” where author CJ Puotinen described it this way:
EMT Gel’s key ingredient, bovine collagen (also described as “a natural medical hydrolysate Type I collagen”), acts as a tissue adhesive, providing a matrix for new cell growth while sealing and protecting wounds and significantly reducing pain, bleeding, scarring, wound weeping, and the risk of infection.
I also have been giving Otto a dose of Benadryl in the morning and at night, to help stop his allergic itching.
Next, I flea-combed Woody; I didn’t find a single flea on him. If fine-coated Coco had a flea on her, I would have seen it walk by; no combing necessary. I’m hopeful that the flea came onto our property on a passing cat or squirrel or something. Nevertheless, I also made an immediate trip to Petco and bought fresh Seresto collars for the dogs. Since fleas aren’t usually a problem for us, I don’t use flea-pesticides year-round, but do use the Seresto collars when we hike in the local areas that are laden with ticks.
As long as Coco is here, Woody’s Seresto collar will have to go on at night and off during most of the day; Coco and Woody chew on each other constantly in play, and I neither want her to get her mouth stuck on his collar or, for a $50 collar, have her chew it off of him (this happened once when I was fostering Odin, another young dog who liked to playfully bite and chew on Woody’s neck and face. $50, down the tubes!).

Fortunately, just a day or two later, the hotspot is healing nicely, and Otto’s licking has ceased. I’m hoping that any other fleas that might have been present were killed before they could have an opportunity to lay eggs. I’ll keep the flea-killing collars on for a few weeks, just in case.
Do you have a highly flea-allergic dog? How do you treat hotspots?

It’s an understatement to say that this isn’t your typical year. However, some things don’t change, and one of those things is the question of what to do with your dog(s) during the holidays. Hanukkah, Christmas, New Year’s, Kwanzaa… these can be stressful times for all of us (especially this year). While most of us probably enjoy having canine family members share the holidays, it can lead to trouble if we’re not careful how we include them in the festivities.
If your well-behaved very social dog loves company and the commotion that can go along with holiday get-togethers, your task is easier. Your primary concern is monitoring their comings and goings so she doesn’t slip out the door as guests arrive and depart. Most dogs, however, are likely to require more management than that. Here are additional things to watch out for:
Counter surfing: Many a dog has enjoyed an unexpected holiday ham that was left unguarded on a counter or table. If your dog has any tendency to help himself to unattended yummies, you need to increase your management mega-fold. If guests are likely to leave surfing-prevention baby gates or doors open, consider parking your dog in a safe room until the chaos subsides.
Stress: Even dogs who are reasonably comfortable with people can be stressed by all the extra activity. Assign one responsible family member to keep a close eye on your dog. If she’s getting stressed, give her a break in a quiet room away from the action, especially if lots of grandkids and/or young nieces and nephews are bouncing about. Unless your dog absolutely adores children, this can be very stressful for her – and stress causes aggression… Enough said.
Holiday Hazards: Some of the things we love about the holidays are deadly to our canine friends, including chocolate, cooked turkey bones, poinsettias, and tinsel. Be extra vigilant about preventing your dog from ingesting items that can harm him – the emergency clinic is not where you want spend your holiday. An excited dog can knock over a menorah or holiday candle and start a fire… also not the way to spend your holiday!
If you want to share any treats with your dog this holiday, here is a list of “human food” safe for dogs.

You love your dog, but (surprise!) not everyone does. If your visitors aren’t going to be thrilled by your Jack Russell’s paws shredding their nylons, or your Bloodhound’s drool decorating their Gucci trousers, be considerate and put Jumping Jack and Drooling Debbie in a bedroom for the evening. If you’re going to be a guest at someone else’s dinner party, be sure your dog will be welcome at your host’s home before plopping Travelling Tess in her canine seat belt and showing up at their door.
If you expect long-term guests – perhaps family staying for a week – and dogs and/or humans will be uncomfortable with repeated close encounters, consider boarding your dog at a well-run facility that you have thoroughly checked out. It could be a lot less stressful for all concerned if no one has to worry about management failures and unhappy results.
Animal professionals generally frown on acquiring new dogs during the holidays – puppies or otherwise, not to mention the ill-advised practice of surprising someone with a pet as a gift. There are exceptions and ways you can make it work.
When I was young, my family did a lot of things wrong with our animal caretaking, but one thing my parents did totally right was surprised me with a puppy for Christmas by wrapping up a collar, leash and dog bowl and putting that package under the tree (best present ever!). After the holiday chaos was over, we had plenty of time to look for a dog. We brought my first Collie puppy home when things were calm and we had time to give him proper care and attention.
If you want to give someone an animal companion as a gift, don’t make it a surprise. Talk to them first to be sure they want to complicate their life by taking on the responsibility for another living being and then let them be part of the process of finding and adopting their new family member. As for the caveat that the holidays are a horrible time to bring home a new dog – that is true much of the time. But if you are home alone for the holidays – no traveling, no family or friends visiting, no parties – it could be the perfect time to add a new canine companion to your family.
Bottom line is – use good judgment. The holidays can be a happy time for you and your dogs if you are careful to make it so.
Featured Image: AleksandarNakic/Getty Images
Read Next: Acorns Can Pose a Danger to Dogs

Some years ago, I read a short piece by one of our long-time contributors, Barbara Dobbins, talking about dogs she knew, including one of her own, who had achieved the age and status to have earned a “permanent hall pass.” I was so charmed by the piece that I asked Barb if we could publish it here as a blog post and she agreed.
At the time it was published, my darling Otto was five years old – in the absolute prime of his well-behaved life. And today, he is 13 years old, and I renew his permanent hall pass every few months, as it gets stained and torn with use.

Don’t get me wrong: Otto is still a Very Good Dog. If dogs are being asked to perform a variety of behaviors on cue and the prize is treats, he can still sit, down, stand, and back up faster than any other canine on the property. He wouldn’t dream of chewing up our human things, or jumping up on people rudely. And he’s always going to be WDJ’s top model – knowing just how to jump up on an object and hit a pose and even find his light.
But there are a number of things that dogs are not allowed to do here in my home or on my property, and Otto has decided, “To heck with it, I’m doing them!” And, precisely because of his long and distinguished record, we now look the other way when he sneaks a cookie off the coffee table, snarfs down the horse poop we come across on the trail, digs in the winter vegetable raised beds, or chases the mail truck along our fenceline, barking furiously the entire time. Oy! That last one is hard for me, especially because I am hosting an impressionable young foster dog who would absolutely love to join Otto in this fun activity (Coco now gets shut in my office at a certain point in the afternoon when the mail truck usually makes its rounds). But he has earned these privileges, in honor of his many years of near-perfect behavior.

I don’t know how much more time I will get with Otto, but I’m not going to spend any of it yelling at or even being annoyed by his new naughty behaviors, that’s for sure.
Do any of your dogs have a permanent hall pass?

I am not a regular reader of or contributor to Reddit.com. But somehow I started receiving “digest” emails concerning dogs – it’s possible I subscribed for some reason that I can’t remember. I guess I can unsubscribe; I hardly ever read them. But every so often, I see a “subject” headline on the email that tempts me into clicking on the digest. Things like:
“Is it possible?”
“Please help, I’m desperate.”
“My vet said she has never seen anything like this in 20 years of practice.”
But it never takes long to click away from the post and all the advice that is offered by (mostly) well-meaning Redditors. Again and again, I find myself mumbling, “Oh for dog’s sake, please hire a trainer!” or “Why are they asking ordinary humans? Why are they not taking that dog to a veterinarian (or another veterinarian)??”
I see this on Facebook, too – people asking for free advice about their dogs on pages devoted to dog training or health. And more recently, I’ve begun seeing dog trainers of unknown education or experience posting training advice for dog behavior problems on Tiktok.
There is a lot of terrific support to be had online and on social media sites – but advice concerning a specific dog’s health, behavior, or general well being that is offered by people without credentials or references should be taken with a block of salt. On any given post, you’ll find (at best) a mixture of (often) conflicting information: good advice (often badly described) side by side with terrible, potentially dangerous advice. Sometimes, commenters will weigh in, “voting” for which tactics seem best and arguing with people voting for the conflicting tactics. Yikes!
I would just like to say: Please don’t solicit advice from the general public about your dog’s health or behavior! It’s rare that genuinely qualified people will offer sound advice for free on the internet – and what’s more, a well educated, experienced professional wouldn’t be caught dead handing out advice to someone without a thorough and individualized intake process that includes many questions tailored to that specific dog and his situation.
If your dog has a mysterious lump or strange response to a food, it’s your responsibility to get him to a veterinarian! If his behavior isn’t what you’d like it to be, don’t ask your friends for advice, but for a referral to a canine behavior professional. Ask why they hired a trainer and whether the trainer’s approach worked to improve their dog’s problem behavior, and whether the dog liked the trainer and the tactics or exercises prescribed by the trainer. And then ask for the trainer’s professional qualifications and experience. It should be more than just professional affiliations; a good trainer will have actual credentials and/or certifications.

When the mercury drops and the snow flies, you can almost hear a swish of canine hearts as they take to the sky. Most, that is, but not all of them. There are dogs that long to avoid even a hint of Jack Frost altogether. While others, look forward to this most wonderful time of the year, age and health conditions can start to make cold a more difficult foe to contend with.
To help our beloved friends we can add an extra layer of warmth for insulation, but when does a dog need a coat?
While it would be phenomenal to simply plug a few variables into an algorithm and find out if our four-legged friends are uncomfortably chilled and at what temperature they would appreciate an extra layer, unfortunately, the result would always be: it depends.

Physiologically speaking, dogs have the ability to maintain their body temperature within optimal boundaries even when the surrounding temperature differs based, in large part, on several factors. Quite literally size matters and when it comes to body heat retention, typically, the bigger the dog, the lower the temperature they will be able to joyfully frolic in. In addition, coat quality, activity level, age, health, and the conditions to which a dog is acclimatized are also important factors.
Nature is full of surprising tricks that can change the equation, however, and rather quickly too.
Should a typically cold-hardy, extra-large Great Pyrenees, who was born and raised in Northern Minnesota, develop diabetes, heart disease, kidney disease, or a hormonal imbalance (such as Cushing’s disease) – physiological conditions that make regulating body temperature a challenge—she very likely would benefit from the addition of an extra layer.

If your dog is cold, their behavior will tell you. They may seem reluctant to go outside, walk very slowly, exhibit whining or barking, even shivering or trembling. Should you share your heart and home with a stoic-dog who will endure pain and hardship without much fanfare, your job is a bit harder. You have to watch closely and look for subtle changes in their typical daily behavior and those that may seem totally unrelated to cold. It can take some sleuthing, but once you identify it, you’ll never miss it again.
The most important thing we can do for our four-legged friends is to become a keen observer, especially as the conditions change outside and within them over time. Like all relationships, developing this awareness takes work, but it’s work that is so worth doing.
Read Next: The Best Dog Winter Coats and Jackets