Writing something for this page is almost always the last thing I do before I send the issue to the printer. This time, though, I was several days away from having the issue completed and working in the wee hours of the morning, when my power went out.
I have a battery backup for my desktop computer, and it gives me a few minutes of power so I can save all the files I’m working on and shut down the computer. But once that was done, I realized that everything I had in progress was trapped on the now-powerless desktop machine. I was tired, but I had been drinking coffee all night, expecting to work for a few more hours. The only thing that wasn’t started already was the editorial. Well, I thought, I have a charged laptop; I can write something before I quit for the night.
I was working in my little office, an outbuilding that’s 50 yards or so away from my house. The laptop was inside the house, and as I got up to walk there, the dogs got up, too, thinking we were all headed inside to sleep, I’m sure.
As we walked across the yard, we all spontaneously stopped. The power outage was affecting my whole neighborhood – there were no electrical lights burning within view – but there was a nearly full moon shining brightly. All three dogs – senior guy Otto, “fun uncle” Woody, and my latest foster project dog, Coco, stood clustered around me, sniffing the air and looking around.
At some point my gaze dropped from the moon and the stars and fell upon the dogs. I watched them experiencing the night with their whole bodies – the chill in the air prickling their skin, the sound of a dog yelping off in the distance – or was it a coyote? – pricking their ears. Their noses lifted as they drank in the scents on the air. Otto puffed his cheeks in and out, eyes shining, gazing toward the neighbor where all the feral cats seem to emanate from. Woody sat down, and then lay down in the gravel. He’s content to do whatever I’m doing, even if it doesn’t make sense. Little Coco shivered a bit and earnestly looked at me for a clue; why are we all just stopped in the middle of the yard in the middle of the night? As she looked up at me, her face filled with concern, her floppy ears flopped backward and upright, which gave her such a comical, flying-fox look that I laughed out loud. And with that, the moonlight spell was broken.
I fetched the laptop and raced the dogs back outside to the office, re-energized and determined to try to share the moment with you. The gifts our dogs give us – the wildlife they help us see, the weather they help us feel, the scents they lead us to, the warmth and humor and companionship they offer us so freely – these gifts have more than enough power to get us through the long dark nights of winter, if we just take a few moments every so often to feel them.
The last time my senior dog, Otto, had a wellness examination, our veterinarian recommended that I start giving him a medication that treats arthritis pain – at least on the days when he exercises more than usual, like when I take him on off-leash hikes. She recommended a newish drug, Galliprant, a nonsteroidal anti-inflammatory drug (NSAID) that works with a slightly different mechanism than most NSAIDs prescribed for dogs, and is supposed to have less of an impact on dogs’ kidneys and livers. I ended up taking home a bottle that contained 30 chewable tablets of the medication.
I’ve been giving the medication to Otto occasionally, on days when we’ve taken a hike, or when he seemed particularly stiff or gimpy in the morning. This has been happening more frequently with the cold weather, and I was down to just a few tablets, so I picked up the bottle the other day to call in a refill.
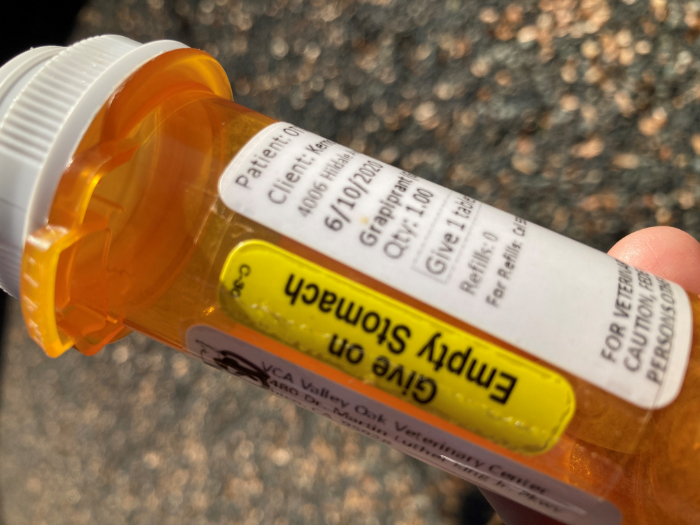
As I waited on the phone for the veterinary receptionist to help me, listening to the clinic’s “hold” music, bottle of medication in my hand, I idly scanned the label, looking to identify the prescription number. To my horror, I saw this:
“Give on Empty Stomach.”
I have been giving the medication to Otto in the morning, with his breakfast – despite a yellow banner on the label that said to give the medicine to him without food.
I don’t know when or why I started giving him the medication with food. Did I not listen to my vet’s instructions? Was I distracted when we were discussing the medication? All I remember hearing is “one tablet given once daily.” Why didn’t I review the label instructions before I gave him any? How could I not notice the yellow label?!
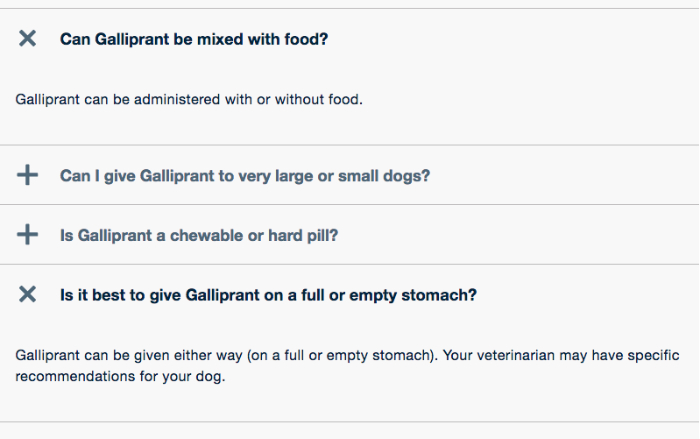
Fortunately, as it turns out, this particular instruction wasn’t critical. When the receptionist came on the line, I told her I was looking for a refill but also wished to speak to the veterinarian briefly about the “empty stomach” instruction. When the doctor became available, she reassured me that the medication could be given either way – but that in her personal experience, she thought it was more effective given on an empty stomach. As long as it was working for Otto, she wasn’t concerned.
Still feeling like a bad dog mom and not to be mollified that easily, I pulled up the drug’s website, which states pretty clearly that it doesn’t matter whether the drug is given with food or not. So now I feel better.
But the issue scared me enough to pass along this advice. Take this opportunity to check the label of any medications your dog receives, right now! Check the dosage and number of pills, the number of times a day your dog is supposed to receive them, and the expiration date (if applicable) of any medication he receives only “as needed.”
Still troubled about my (as it turns out, harmless) screwup with Otto’s medication, I mentioned my error to a couple of friends – and one admitted she once, a few years before, dosed her dog with half of the medication that the label called for, at least half-way through the bottle. It was a two-week prescription, and only when it seemed like the bottle wouldn’t be empty in a week’s time did she examine the label more carefully. The dog was supposed to get two capsules, twice a day, and she had been giving only one capsule twice a day. She admitted her error to her vet, who told her to come and pick up more of the medication, so the dog could receive the full dose for the entire recommended period, as a half dose wasn’t likely to be effective.
CBD “supplements” for dogs come in many forms; the most common are liquids that are meant to be administered from a syringe or dropper, and liquid that has been mixed into edible treats or chews.
In December of 2018, the Agricultural Improvement Act of 2018 (2018 Farm Act) was signed into law. It removed hemp, defined as Cannabis sativa L. with less than 0.3% dry weight of the psychoactive cannabinoid substance Delta-9 tetrahydrocannabinol (THC), from the definition of marijuana in the Controlled Substances Act (CSA). This legislation removed significant research barriers for both academic and commercial research into cannabidiol (CBD), as well as legal barriers for growing and harvesting these plants and the refining and selling of products that contain CBD to the public. CBD has been advocated for use in a wide range of conditions in dogs from anxiety to epilepsy to cancer. But other than a handful of small-scale studies looking at the use of CBD oil in dogs, there is no data on veterinary usage. Most of the available information is individual case studies and/or anecdotal.
In Whole Dog Journal’s July 2019 article “Know Your CBDs,” author Catherine Ashe, DVM discusses the three main studies on CBD that were available at that time. Even today there are still very few publications on the efficacy of these products in clinical conditions. But this is not due to the lack of scientific interest in CBD applications; researchers are looking at it from a variety of angles: Is it effective? How does the canine body absorb, synthesize, and metabolize CBD (aka pharmacokinetic analysis)? What is the recommended dosage for different ailments in canine patients?
Research can take a long time – sometimes, many years! Potential veterinary drugs must undergo examination at a variety of levels to evaluate efficacy and safety. And it’s only been two years since the Farm Act lifted the restrictions that prevented earlier research on CBD. But fascinating and important results are beginning to trickle in.
Necessary foundational research for the growing field includes two new studies that evaluated the pharmacokinetics and safety of CBD use in dogs. Overall, both studies found that CBD was well tolerated with a favorable safety profile.
Vaughn D, Kulpa J, Paulionis L. Preliminary investigation of the safety of escalating cannabinoid doses in healthy dogs. Front Vet Sci. (2020) 7:51. Overall, the study concluded that dogs tolerated dose escalation of a CBD product well, experiencing only mild adverse effects. It also provided comparative evidence that CBD was safer and more tolerated than doses containing higher concentrations of THC.
Fernandez-Trapero M, Perez-Diaz C, Espejo-Porras F, de Lago E, Fernandez-Ruiz J. Pharmacokinetics of Sativex(R) in dogs: towards a potential cannabinoid-based therapy for canine disorders. Biomolecules. (2020) 10:279. The study investigated Sativex®, a phytocannabinoid-based medicine marketed for the treatment of spasticity and pain in human multiple sclerosis patients, for use in canines for the treatment of central and peripheral pathological conditions. The study found that single dose or a multiple dose sublingual administration of Sativex® to naïve dogs was well-tolerated and produced the expected pharmacokinetic profiles, resembling the results of those published in previous pharmacokinetic studies.
Another original research article published this year looked at how CBDA, the acidic precursor to CBD, functioned in comparison to CBD, THC, and THCA, the acidic precursor to THC. Many products contain small amounts of all four compounds; it has been widely thought that CBDA has great potential as a stand-alone compound as well as in conjunction with CBD. Prior to this study, CBDA has not been the subject of much research. This study was funded by ElleVet Sciences and used an ElleVet product. Spearheaded by Dr. Joseph Wakshlag of Cornell University College of Veterinary Medicine with the assistance of colleagues from the University of Florida, the investigation determined that CBDA is both more readily absorbed and retained in dogs when compared to CBD, particularly when administered with a lecithin-based delivery oil. CBDA is shown to be anti-inflammatory, and this superior absorption and retention offer great promise in veterinary use.
Wakshlag, J, et al. Pharmacokinetics of Cannabidiol, Cannabidiolic Acid, Δ9-Tetrahydrocannabinol, Tetrahydrocannabinolic Acid and Related Metabolites in Canine Serum After Dosing With Three Oral Forms of Hemp Extract. Front. Vet. Sci. (04 September 2020).
Two recent studies evaluated the use of CBD for treating osteoarthritis pain in dogs:
Researchers from Baylor College of Medicine in collaboration with CBD brand Medterra conducted a 4-week, randomized, double-blind, placebo-controlled study with 20 large dogs diagnosed with osteoarthritis. Each dog was randomly assigned to receive either a placebo or one of three different CBD options. The study found that CBD significantly decreased pain and increased mobility among the dogs receiving the higher doses of CBD or received it in a liposomal formulation. No significant adverse effects were observed. In comparison, the placebo group and low CBD group showed no improvement. Because those dogs in the higher dose group still showed improvement 2 weeks after ceasing the administration of CBD, it is suspected that the CBD was addressing the underlying inflammatory issues.
Verrico, C, et al. A randomized, double-blind, placebo-controlled study of daily cannabidiol for the treatment of canine osteoarthritis pain. PAIN. (September 2020) 161:9; p 2191-2202.
Scientists at Colorado State University conducted a 90-day pilot clinical trial to assess the impact of a full-spectrum product containing hemp extract and hemp seed oil on 37 dogs with chronic maladaptive pain (primarily as a result of osteoarthritis). Thirty-two dogs completed the study, of which 30 showed evidence of improved pain management. At the time of enrollment, 23 dogs were taking gabapentin; with the addition of CBD, 10 of those dogs were able to discontinue the gabapentin and an additional 11 were able to have their daily dose reduced.
Kogan, L., Hellyer, P, Downing, R. (2020). The Use of Cannabidiol-Rich Hemp Oil Extract to Treat Canine Osteoarthritis-Related Pain: A Pilot Study. AHVMA. (Spring 2020) Volume 58.
Also out of Colorado State University, which is leading a great deal of the veterinary research on CBD, is a study that investigated the effects of CBD on the cells of canine and human glioblastoma (an especially virulent form of brain cancer). The experiment “showed that CBD slows cancer cell growth and is toxic to both canine and human glioblastoma cell lines. Importantly, the differences in anti-cancer affects between CBD isolate and extract appear to be negligible.” The anti-cancer effects of cannabis are still not understood, but this study suggests that CBD can damage the mitochondria of cancer cells. It is hoped that “this study will lay the groundwork for future preclinical studies and randomized controlled clinical trials in order to provide evidence for effective Cannabis treatments for many cancer subtypes.”
Baram L, et al. The heterogeneity and complexity of Cannabis extracts as antitumor agents. Oncotarget. (2019) 10: 4091-4106.
Clinical Trials:
Efficacy of Cannabidiol for the Treatment of Epilepsy in Dogs (recruiting phase)
The aim of this study at Colorado State University Veterinary Teaching Hospital is to assess the efficacy of CBD in treating canine epilepsy. Each participating dog will be randomly assigned to receive either CBD or a placebo for 12 weeks and then switch to the opposite medication for an additional 12 weeks.
Coming Soon: Purdue University College of Veterinary Medicine “Effect of CBD Products in Canine Anxiety”
Other Research to Watch:
Canopy Animal Health, is conducting research on the safety and efficacy of CBD in companion animals at academic and private research centers in both Canada and the United States, as well as actively investing in CBD research to treat anxiety, epilepsy, symptom management of chemotherapy, osteoarthritis, and joint pain and inflammation.
This is a guest blog post that touched us deeply. Its author, Jenny Efimova, KPA CTP, is the founder and owner of Dogminded. Efimova offers private dog training in and around Boston, Massachusetts, as well as virtual training for puppies and dogs and their humans. One of her mottoes: “How we teach dogs matters as much as what we teach them.”
Yesterday I shared a few stories on my Instagram page about the false belief that showing our dogs affection and allowing them on the couch or bed may cause behavior problems, including separation anxiety. Since then I’ve received *dozens* of messages from people expressing relief and gratitude and sharing how guilty they have been made to feel for treating their dogs with basic compassion and kindness.
This is heartbreaking and I want to reiterate a few things: One, dogs are social animals who have uniquely evolved to live with and alongside us. Social contact is a *basic need*. They seek comfy places next to their humans for no other reason than that they like comfy places next to their humans.
Not allowing your dog on furniture, ignoring your dog, or rationing how you show your dog affection does not provide “structure” or help resolve behavior issues. This is magical thinking, something that we compensate with when we lack adequate education and skillset to address behavior issues with science and evidence-based interventions. And in the year 2020 it does not have a legitimate place in the world of dog training and behavior.
It’s also abject cruelty and ignorance to advise people to withhold attention, affection, and comfort from their dogs who are already suffering. Separation anxiety, for one, is a disorder not something that results from too many cuddles or access to the couch.
Blaming people for their dogs’ behavior problems they did nothing to cause is especially egregious and has to stop. People don’t deserve to carry this guilt, nor should they be made to shun their dogs and treat them in ways that are contrary to the very reasons we bring dogs into our lives.
Dog training is an unregulated industry and the information you find is not created equal. So please beware of advice from self-proclaimed experts on social media, vet your sources, and follow your instincts when something feels wrong.
I’ve been there and if you have too, you know exactly the feeling I’m talking about. It’s the sense of moving through your own discomfort because a “professional” told you so. I know we can do better than this. Our dogs deserve better.
The acorns themselves are toxic if consumed by dogs. Underfoot the acorns (and particularly their caps) make it impossible to walk on the lawn barefoot.
Not that anyone asked, but my favorite tree in the whole world is the oak tree. We have dozens of species of oaks in California, and where I grew up, in the great Sacramento Valley, the Valley Oak (Quercus lobata) is the most ubiquitous and also the largest oak tree around. They live to be hundreds of years old and grow into massive, photogenic shapes. When my husband and I bought the property where we have lived for the past (almost) three years, one of the key selling points was the magnificent hundred-year-old Valley Oak that stands in front of the house, and several other smaller Valley Oaks sprinkled around the property, along with some lesser oak varieties, the Blue Oak and the Live Oak.
Here’s the down side of living with oak trees, one that I never fully appreciated until now: acorns. So. Many. Acorns. And while all the oak trees are producing them, the Valley Oak makes some of the largest ones; they exceed the size of a standard tube of lip balm. Their distinctive “caps”, too, are a hazard. When they separate from the acorn, they become a separate large, hard, marble-shaped hazard.
The Valley Oak in our front yard: Magnificent and a prolific producer of acorns
Acorns underfoot on the lawn. (“Ow! OW!”)
Acorns getting mowed by the mower (turning the mower into a dangerous, projectile-throwing machine).
And worst of all: Dogs chewing on and (sometimes) eating the acorns.
California kids grow up with the information that the native indigenous people in California harvested the acorns and made them a staple of their diet – and every California kid who lives near an oak tree tries to reenact this. You gather acorns, peel off the skin to expose what appears to be a big, delicious nut, and find some rocks capable of grinding the nuts into a coarse flour. The goal is to then add some water and use your hands to mix the flour and water into a dough and try to make a tortilla. At some point in the process, you dip your finger into the flour and lick it, or take a little bite of the dough, and – ACK! Blech! It’s bitter!
When California kids get a little older, they learn that acorns are full of bitter tannins, and that the native people used to leach the flour with water, sometimes many times, to remove the bitter substance and make the acorns safe to eat.
And, as vet-bill-paying adults, we learn that in addition to being bitter-tasting, these tannins can be toxic to humans, horses, and dogs. Shoot!
Tannins in acorns can be toxic to dogs
I know several people whose dogs get sort of addicted to chewing the bitter-tasting nuts and end up with an extremely upset stomach – and in severe cases, kidney failure and death. A dog who becomes inappetent after eating acorns requires immediate veterinary care. My sister had a little dog who, at least once a year, would require a vet visit after sneaking a few acorns. She liked them after it had rained a time or two in the fall, when the nuts have gotten soaked with rainwater and fermented slightly – which seemed to increase their toxicity.
It took me about 10 minutes to collect this bucketful of nuts and caps.
Despite the wealth of nuts littering my property in the fall, neither of my dogs has been interested in picking them up or chewing them, even speculatively, and up until now, neither have any of my foster dogs. That is, until my most recent foster dog arrived. I have to keep a very close eye on Coco, who has become inexplicably drawn to chewing on the acorns, to the extent that I basically can’t have her out of my sight on my fenced, two-acre property. Wah!
Like my sister’s dog from years ago, Coco is (thankfully) uninterested in the dry ones that cover most of my property, and is mostly drawn to the ones that have been soaked by the sprinklers on my front lawn. While this is quite a lot, given the GINORMOUS Valley Oak, the pride of our property, at least it’s just those. So it’s my new evening hobby: hanging out on the front lawn in the evenings with my dogs, throwing the ball for Woody, watching Woody and Coco wrestle, watching Otto watch for feral cats and squirrels … and picking up acorns from the lawn, and dumping them in our “green waste” barrel. I probably have a few more weeks to enjoy this new hobby before the tree’s supply is done and I can relax again.
Have you ever had trouble with an acorn-eating dog? Spread the word about this danger.
This darling little hound-mix joined the family for four days, recuperating from neuter surgery on my watch before being picked up by his new family.
Last week, I “fostered” a dog for four nights – not a big deal. He was a hound-mix, about a year old, who had been languishing in my local shelter for too long. A bit of an oversight, actually, due to the fact that the shelter has been crazily preoccupied with taking in and caring for dozens of animals who were evacuated or rescued from a month-long wildfire event. This little hound had the luck (or misfortune, depending on how you look at it) of being brought into the shelter within a day of the large evacuation necessitated by the fire’s rapid progression into our community, and he got a little lost in the shuffle of animals with more dramatic needs.
I spotted the little guy when volunteering at the shelter to help with the fire-evacuated dogs. (The ones that had been brought in as “strays” by first responders in the fire zone needed good photos taken for identification purposes, in hopes of reuniting them with owners; I also made phone calls to the owners of dogs that the shelter was holding for safe-keeping – people whose homes had burned down – to gently inquire whether they had made any progress in finding housing.) The shelter’s regular adoption program has been on hold off and on for months, first due to COVID, and now due to the formidable needs of animal fire victims.
But I had received an email from a friend of a friend of my son, asking for help in finding a family dog. And because of that specific pedigree (my son’s friend and his fiancée have adopted TWO dogs from my shelter, and I get to see the dogs’ new, wonderful lives in my Instagram feed), I said I’d help, and immediately thought this family and that little hound would be a great match – even though the family lives a good two-plus hours away. I implored them to come meet the hound as soon as possible and then met them at the shelter on a Sunday (when only the cleaning staff is present).
As I knew they would, they fell in love with him. I pressed to get the hound admitted for the next possible surgery date for neutering and took him home after his surgery, to wait for the next date his new family could come to adopt him. It was just four nights later.
But for me, it takes even less than four nights to form all sorts of opinions about how a dog should best be handled and cared for. Whenever I foster, I find myself trying to stuff all sorts of information into the adopters’ heads before they drive off with my ex-foster dog. And I kick myself, time and time again, when I think of things I meant to mention to them before they left – more than once, I’ve sent new owners emails about their new dogs before they’ve even gotten home with their new pets!
And then there are the general dog-care and dog-training tips that I wished all dog owners would know and employ. Some day, when I have a little extra time, I’m going to formalize all of them into a little booklet that I can send home with adopters. As I drove home from the shelter last Sunday, mulling over whether I had told Arlo’s new family “all the things,” I decided that, in an effort to jump-start that project, I’d at least write a blog post with a few notes about what I’d most want them to remember – and ask you for your top dog-care tips. What two or three things do you insist that your friends or puppy buyers or new adoptive families know?
My top tips for new dog owners
Here are a few of mine:
Keep ID on the dog at all times for at least the first few weeks before you remove it, even for just a bath! And even if there is ample evidence to the contrary, pretend like your new dog may try to escape at any moment. Don’t leave doors or gates not-quite-closed. Don’t take it for granted that he will follow you from the car to the house or vice versa; use a leash whenever he’s not securely contained. Don’t leave the house with windows open; lock the yard gates so the kids can’t accidentally forget to latch them. Practice this diligence until it’s clear that your new dog knows and is comfortable with you, knows where he lives, recognizes the sound of your car, and is well-started on a positively reinforced recall.
“Arlo” and his new family.
Hand-feed him for the first few days. Take every opportunity to reinforce his concept of you as the most enjoyable human ever.
That said, don’t let him do the things you don’t want him to do, from the very first day. If you don’t want him on the couch or beds, don’t let him on the couch at all. If he hops up, throw a toy or treat across the room to lure him off the couch, and then either block him from jumping up again, and either sitting on the floor or next to his dog bed with him until he relaxes there, or putting him in a crate or on a tether with a nice fresh raw meaty bone or food-stuffed Kong toy. In other words, give him an equally enjoyable option!
Also, start teaching him to be alone in short bits from day 1. Give him a food stuffed Kong or chewy and leave him alone, crated or closed in a secure and comfortable room, for just a minute here and there. Observe how he handles this. If he notices you leave and goes back to sleep, that’s awesome. If he leaps to his feet and compulsively follows you every time you leave the room, you are going to need to work on this sooner and more formally. (See this article on why and how to prevent and deal with separation anxiety and isolation distress.)
Take him outside to potty a lot! At least once an hour! Praise him and give him treats or petting (if he likes that) every single time he “goes” outside. And watch him constantly, actively, when he’s inside. Try not to give him a single opportunity to “make a mistake” and “go” inside. If you screw up and he does go potty in the house, take a rolled up newspaper and hit yourself over the head and say, “I must pay better attention!”
Don’t be in a rush to take him everywhere! Let him get to know you and your family and home for at least a few days! And don’t overwhelm him with visitors at first! As excited as you and your family may be, remember that the change is very overwhelming and stressful for your new dog. He’s trying to figure it all out. Give him a little time.
Don’t take anything for granted. Assume he knows nothing about living with humans. Don’t leave food on the coffee table, your child’s desk, or even the kitchen counter. Put your kitchen and bathroom garbage cans out of reach. Make sure the cat or other small pets in the house are kept safely and securely separated when no one is actively supervising the dog.
If that new owner is off to the pet supply superstore, my top tips would be: No plastic dishes! Stainless steel bowls only. Beds: As thick as possible. Treats: Don’t buy them; use tiny bits of cheese, lunch meat, roasted chicken, etc., instead. No Flexi-type leads! No store-bought rawhide or “chewies.” (There is exactly one supplier of rawhide that I trust, and I buy only one product they make – for all dogs, no matter their size.) Toys: Lots!
If you had to turn over a dog you loved to a new home, what are the bits of advice you’d most want to convey?
Our test dog works to eat around a slow-feeding device called the Gobblestopper. (The GPS tracking device he's wearing on his collar is being tested for a product review that will appear in the next issue of WDJ)
Can your dog make an entire bowl of food disappear faster than you can say, “Bon appétit?” Has he ever inhaled a bowl of food so fast he vomited it back up a few minutes later? Does her seemingly frantic consumption lead to gagging or choking?
If any of these scenarios sound familiar, it’s wise to check out one of many commercially available slow feeders or experiment with creating one yourself to help your dog dial down her speed-eating ways.
Eating too fast can lead to gagging and choking – plus, speed eaters tend to gulp air as they execute their deep-dive into the food bowl. This excess air can interfere with digestion, cause gas, and even lead to gastric dilation and volvulus, commonly known as “bloat,” a potentially fatal condition where the stomach fills with excess gas and flips on itself, restricting blood flow and requiring life-saving emergency surgery.
Slow-feed bowls and other tools also can help turn mealtime into an opportunity for enrichment. When using a slow feeder, your dog can tap into his problem-solving abilities as he maneuvers the device. This engages his brain more than when simply diving face first into an open bowl of food. Mental exercise is just as important as physical exercise in creating a well-rounded canine companion.
The ability to slow a dog’s eating is also critically important to the success of certain training protocols. For example, when working with a dog who tends to guard his food, it’s helpful if he’s eating slowly enough to give us time to implement some behavioral interventions.
A common positive-reinforcement approach to working with a dog who guards his food is to pass by the dog as he eats and drop a food item considered “better” than what’s in his bowl; this helps to counter-condition how the dog feels about a human approaching his food. However, if the dog inhales the contents of the bowl before you can approach, this is difficult to accomplish!
Who Needs a Bowl, Anyway?
While slow-feel bowls are helpful, another approach to slowing a speed-eater is to ditch the bowl all together in favor of stuffed food puzzles, planned scavenging opportunities, or even hand-feeding via training.There’s no rule that says dogs must eat meals at set times, and from a bowl! Often, high-energy dogs benefit from a “sit quietly and color” activity such as extracting part of a meal from a well-stuffed, frozen Kong or a Toppl toy, and it’s easy to split a dog’s daily ration of kibble into three or more puzzle toys to be offered at different times throughout the day.
Snuffle mats allow dogs to fully engage their sense of smell as they poke around the fabric strips in search of kibbles. You can even offer a wide-spread kibble scatter out in the yard as if you’re feeding chickens! (Admittedly, these last two techniques work better with kibble than with home-prepared or raw diets, but these work well in Kongs and Toppls.)
And of course, there’s training time! On busy training days, my dogs have always eaten very little from a bowl. Rather, I’m leveraging their daily caloric intake in an effort to generously reinforce desired behaviors – especially when working with them as young puppies.
Don’t be afraid to ditch the dog bowl in favor of more creating feeding strategies that support your training goals and the development of a harmonious household!
SPEED TESTS
We selected five commercially available products that are marketed as able to slow a fast eater. We timed how long it took our test dog, Saber, an 8-year-old Golden Retriever, to navigate each bowl. Each timed trial was compared to his baseline of 2:00 to eat a meal consisting of two cups of kibble with a small amount of water (to dissolve a powdered supplement) from a regular stainless steel dog bowl.
We recognize our test dog’s standard approach to a bowl of food doesn’t necessarily qualify as “speed eating” – many of you may have even faster chow hounds – but he’s in no way a “picky eater.” He dives into the bowl, eats with enthusiasm, and doesn’t leave the bowl until the food is gone.
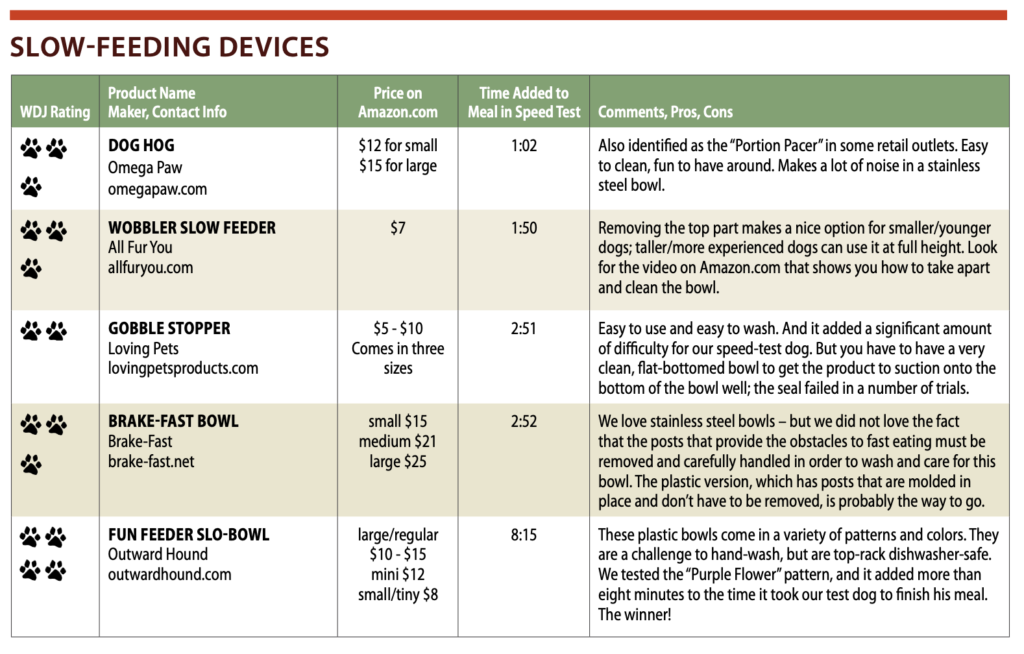
Beyond timing how long it took to empty each bowl, we also considered cost, materials, ease of use, and how easy each product is to clean. Hungry to know more? Here’s what we discovered, listed in order of least to most additional time needed to finish a meal.
DOG HOG
Dog Hog
The Dog Hog is a weighted stainless steel ball, reminiscent of those gazing balls popular in backyard gardens in the early 1990s. It comes in two sizes: The small Dog Hog measures 2.88 inches in diameter and weighs six ounces and the large measures 3.5 inches and weighs 8 ounces.
The Dog Hog is super easy to use. Simply place it in your dog’s bowl and add food around it. The smooth, slippery nature of the Dog Hog makes it difficult for a dog to be able to successfully lift it out of the bowl in order to better reach and gobble the food. Its weight makes it challenging to shove it out of the way. It’s certainly not so heavy that it can’t be moved, but in our test, it wasn’t easily chased around in the bowl by an enthusiastic snout.
It should be noted that sound-sensitive dogs may not appreciate the sound of the stainless steel ball rolling around in a stainless steel dog bowl.
Its simple design gives Dog Hog high marks for ease of use both in the bowl and when it’s time to clean the device. However, it added only 1:02 minutes to the time it took Saber to finish a meal, bringing his total eating time to 3:02.
WOBBLER SLOW FEEDER
Wobbler Slow Feeder
As I unpacked the Wobbler, I was reminded of the classic 1970s childhood toy and its jingle, “Weebles wobble but they don’t fall down!” This fishbowl-shaped slow feeder functions in much the same way; it can be pushed over in all directions, but thanks to its weighted silicone base, it rights itself as soon as it’s released. You pour your dog’s food inside the fishbowl, er, bowl, and your dog has to put his head inside it to chase the food around the inside of the bowl.
The Wobbler stands about 5.5 inches tall, is about 4 inches deep, and has a 5-inch opening. The top 2 inches can be unscrewed and removed, reducing the Wobbler’s overall height to 3.5 inches, but more importantly, reducing the depth to just 2 inches and increasing the diameter to 6.5 inches. This is great for smaller dogs – or any dog who might be leery about lowering his head into a relatively small space.
The bottom half of the Wobbler sphere has an interior bowl with a series of ridges inside, creating channels around which the kibble falls. This interior bowl spins within the external sphere, but when we spun it by hand, we felt a fair amount of friction, so we’re not quite sure how much, if any, spinning happens as the dog eats.
When it came time to clean the bowl, we couldn’t figure out how to remove the internal bowl, and were ready to just chuck the product altogether. Cooler heads prevailed, however, and WDJ’s editor pointed us toward a video on the Wobbler’s Amazon page that showed how it can be done. Okay! It was back in the test.
According to the manufacturer, the Wobbler holds up to four cups of food, is made with food-safe plastics, and is BPA-free. We appreciate its unique ability to adapt to both large and small dogs.
The Wobbler added 1:50 to the time it took Saber to finish a meal, bringing his total eating time to 3:50.
GOBBLESTOPPER
Gobblestopper
When we selected products to review, “ease of use” was one of the attributes we looked for, and the Gobblestopper looked very easy to use, so we gave it a try.
The Gobblestopper consists of a molded plastic bone on a one-inch base that suctions onto the bottom of any flat-bottomed dog bowl. The dog has to eat around the obstruction and use his tongue to sweep the food out from under the bone.
We used the Gobblestopper in a stainless steel bowl with an interior diameter of 7 inches, which left about 1 to 2 inches of space between the device and the walls of the bowl. It took Saber an extra 2:51 minutes to finish a meal, bringing his total eating time to 4:51.
We did run into an issue with the suction cup not sticking well to the bottom of the bowl, and near the end of the meal, we noticed it was being pushed around as Saber worked to extract the final kibbles. The suction cup itself is extremely shallow, which likely makes it difficult to achieve a strong seal. Adding water to Saber’s food may have also lessened the strength of the seal.
Had the suction cup done a better job, we’d give the Gobble Stopper higher marks, as it’s easy to use, easy to clean, and more than doubled the amount of time it took our test dog to eat a meal. Unfortunately, given that it sometimes fails to stick to the bowl for the duration of the meal, we’re less enthusiastic about recommending it.
BRAKE-FAST BOWL
Brake-Fast
Many people prefer stainless steel bowls for their non-porous quality, so we were happy to add a stainless steel slow feeder to our roster. The stainless Brake-Fast Bowl is essentially a standard dog bowl with three removable posts around which food is added. This bowl is available in small (1 quart), medium (2 quart) and large (3 quart) sizes. We tested the 2-quart bowl.
With more than 2 inches between the posts themselves, admittedly, we weren’t expecting much in terms of challenge, so we were surprised to discover it added nearly 3:00 to our test dog’s eating time, increasing the total eating time to 4:52!
Interestingly, we noticed Saber tended to pick up and chew bites of food more often using this bowl compared to other bowls, and kibbles positioned between a post and the side of the bowl seemed especially challenging to extract. The Brake-Fast bowl has a non-skid edge, but it did slide a little as Saber worked to get the final few pieces of food.
While we loved the unexpected challenge this bowl provided for Saber, we were less than thrilled to discover that the product comes with five-part cleaning instructions.
Per the manufacturer, to properly clean the bowl, one must first unscrew the posts, hand wash all parts with warm soapy water (while taking care to not submerge the posts), dry thoroughly, and then reattach the posts without over-tightening. That’s a lot of steps!
The company also makes a plastic Brake-Fast bowl with molded permanent stanchions, and, as much as I like stainless steel, I think I’d prefer the simplicity of hand-washing the plastic version that doesn’t have to be taken apart and put back together for cleaning.
DIY Slow-Feed Bowls
Chances are, you already have items around the house that can be repurposed to create a slow-feed bowl for your dog. Try experimenting with one of these DIY alternatives to a commercial slow-feed bowl:
* Add a small, upside down terracotta pot to your dog’s dish. The pot placement creates a “moat” from within which the dog works to extract the kibble. Similarly, you can add a large rock to the center of the bowl. (To protect his teeth, make sure the dog doesn’t try to pick up the rock.)
* Turn a muffin tin into a meal puzzle. Add varying amounts of kibble to each of the individual muffin cups. Top cups with dog-approved items to be removed first, such as a tennis ball or Kong toy.
FUN FEEDER SLO-BOWL
Our winner in the slowing-down-the-dog contest? The Fun Feeder Slo-Bowl, which added a whopping 8:15 to the time it took Saber to finish a meal, for a total eating time of 10:15!
Fun Feeder Slow-Bowls
The Fun Feeder comes in three sizes, five colors, and four challenging designs. We tested the Large/Regular “Purple Flower” Fun Feeder, which is 11.75 inches in diameter, two inches deep and holds up to four cups of food. The mini Fun Feeder of the same design is 8.5 inches in diameter, 1.75 inches deep and holds up to two cups of food.
This entire feeder is a complex challenge; there’s not a single area of the bowl that appears to create the opportunity for an easy-grab bite. The widest part throughout the interior of the design is only about 1 inch, making it nearly impossible to reach in and “bite” a mouthful of food. Rather, it seems food must be scooped into the mouth using the tongue as a spoon. If you need to really slow down a dog, this seems like a good option.
My dog would probably be happy to know that the bowl createdchallenges for me, too. I add a powdered supplement to Saber’s food, and mix it into his food with a little water, but because this slow-feeder doesn’t have any bowl-like area in which to mix the supplement into the food, I had to use a separate bowl for mixing, and then dump it into the Fun Feeder, scraping as much of the (expensive!) supplement off the sides of the first bowl. Kind of a pain.
Also, the narrow channels made it difficult to hand-wash, but per the manufacturer, it’s top-rack dishwasher safe. It’s also free of PBA, PVC, lead, and phthalates.
VARIETY, SPICE OF LIFE
I’ve always been a fan of food puzzles for dogs, especially young puppies. All of my dogs have consistently eaten at least some of their daily ration of food out of frozen stuffed Kongs or Toppl toys, or from a snuffle mat of some sort.
While I’m not worried about the general speed with which Saber eats his meals, I’ve still chosen to keep the Dog Hog, Wobbler and Fun Feeder in weekly rotation to add a little extra variety, and hopefully, mental stimulation to what can be an otherwise very predictable dining experience.
Many dogs will "work" for ordinary kibble or cookie-style treats at home, but need a higher-value treat in order to focus on you and your cues when in the face of a more distracting (or more stressful) environment. And some dogs get too stressed in public to take any treats, no matter how meaty and delicious. Finding a non-food reinforce is critical for training these dogs.
I use treats when I train. So do my clients. Now that positive reinforcement training has a 25-year-plus track record in the dog world (supported by studies that affirm its effectiveness), the use of treats in training has become widely accepted and embraced.
There are times, however, when you can’t use treats. Perhaps your dog isn’t particularly motivated by food. Maybe there’s a medical reason your dog can’t have food right now. Or perhaps (horrors!) you ran out of treats. The good news is that food isn’t the only form of reinforcement we can use in training – there are a number of others ways you can reinforce your dog’s behavior.
How to train a dog that’s not food motivated or without treats
When, on a leashed walk, this little dog sees other dogs, he gets so stressed that he loses all interest in food treats of any kind, regardless of value. Only when the other dog is at a greater distance will he relax and calmly take food.
The fact is, all dogs must be food motivated, at least to some degree, or they truly will starve. We all have to eat to live.
But it’s true: Some dogs are more interested in food than others: Labrador Retrievers are notorious for being “food hounds.” In fact, a recent study found this breed is more likely to have a very strong interest in food because they have a specific gene mutation associated with food obsession. (Flat-coated Retrievers have it too, but it has not been found in any other breeds.) Still, all dogs must eat, so the first questions we need to ask are:
Why is my dog not more interested in training treats?
Are there things I can do to increase my dog’s interest in training treats?
If I can’t get him to be more interested in treats, or if he can’t have treats right now for some reason, or if, inexplicably, I ran out, are there other reinforcers I can use in my training program?
There are several reasons why your dog might not appear to be motivated by food during training:
Medical causes. We always want to consider and rule out or treat any possible medical causes for or contributors to a behavioral challenge, including anorexia. If your dog truly has little to no interest in food, if you have not already, please discuss this with your veterinarian as soon as possible. There is a long list of possible medical reasons why your dog may not be interested in food, and some of them are very serious.
Treats are low in value to your dog. Perhaps you’ve heard the suggestion to use your dog’s regular kibble for training. This could well work for a Lab and for other very food-focused dogs, but for dogs who aren’t as interested in food, kibble just might be too boring.
Easily bored with your high-value treat. Some dogs get bored with (or just too full to be very interested in) a great number of the same delicious treat. Be prepared with a list of treats your dog considers high-value, and when her interest in one starts to wane, switch to another.
Most dogs love chicken (baked, boiled, or thawed-out frozen chicken strips), and yet we often see dogs tire of it at our academies, where they are plied with training treats throughout the day. Other treats dogs tend to love include roast beef, cheese, cooked hamburger, meatballs, peanut butter squirted from a tube, ham, baby food – the list is endless. If your dog is less than enthusiastic about food, the longer your list of potential high-value treats needs to be.
Your dog is easily distracted, or the environment holds too many or too highly disturbing distractions. If your dog is on the mild-to-moderate end of the food-interest continuum, environmental distractions can serve to deflect her desire for treats, especially if she is easily distractible, and/or if you haven’t done your homework to generalize her behaviors to a variety of different locations. If this is the case with your dog, try higher-value treats and/or do more training in a less distracting environment before generalizing to more distractions. (Your backyard might seem perfect – but not when there are squirrels racing around the trees, or the neighbor’s dogs are barking at you through the fence.)
Your dog is not hungry. This is a concept totally foreign to your average Labrador, but a lot of dogs who are not as crazy about food as the Lab will be less enthusiastic about working for treats if they just finished a meal. This is an easy fix: Schedule your training sessions before mealtimes, not after, and don’t feed your dog just before training class.
Your dog is stressed. This is one of the most commonly overlooked reasons for dogs to turn up their noses at their training treats. It is biologically appropriate, for survival reasons, for her appetite to shut down when your dog is stressed. When the brain signals “danger,” the last thing an organism should do – if they want to survive – is stop for a bite of food, so the part of the brain that controls appetite turns off until the danger is over.
If your dog is reluctant to take treats because she is stressed, you may be able to tempt her with higher-value treats, but the best solution is to figure out how to make the stress go away – or at least decrease enough so she can happily eat again. (If she can normally take a treat gently, but in a stressful situation goes from not taking the treats to blindly grabbing at the food, sometimes getting your fingers in the process, her stress level is still too high for effective learning; move farther from the stressor.)
Sometimes a dog will learn to take treats in the face of her stressor just through habituation (she just gets used to it), although a concerted effort at counter-conditioning and desensitizing her to the stressor tends to be more effective and faster. (See “Counter-Conditioning and Desensitization,” WDJ March 2020.)
In some cases, if the dog’s stress levels are persistent, behavior modification drugs are in order. This calls for another discussion with your vet. If your veterinarian is not behaviorally knowledgeable, she can schedule a phone consult with a veterinary behaviorist for assistance in determining what medication(s) might be appropriate for your dog. Your vet can find a list of Certified Veterinary Behaviorists at dacvb.org/search.
Positive reinforcers for dogs (that aren’t food)
Nova is excited and she wants to race around and smell the grass. Jessie asks her for some basic behaviors of a fairly short duration – like this bit of loose-leash walking – and then uses the chance to sniff the grass as reinforcement. Jessie marks Nova’s nice eye contact on a loose leash with a “Yes!” and then releases Nova with a “Go sniff!” cue.
After a bit of sniffing, Jessie will ask Nova to walk with her again. By asking for short sessions of calm, attentive behavior, which is reinforced by a tiny bit of freedom to explore, they are able to traverse the field without Nova getting overexcited by total freedom or frustrated by too much tight control and no opportunities to check out her surroundings.
One of the great things about using food as a reinforcer in training is that the dog can eat the treat quickly and immediately go on to the next behavior. But anything your dog perceives as “good stuff” can theoretically be used as a reinforcer. Play, for example, is an excellent, very strong “other” reinforcer for many (but not all) dogs. Keep in mind, however, that other reinforcers can take more time to deliver and regroup from, and thereby are more likely to interrupt the flow of training.
Now that the use of food in training has become so widespread, it’s easy to forget that there are a multitude of other ways to reinforce your dog’s behavior.
The definition of a reinforcer is “something that causes a behavior to increase.” In positive reinforcement training we teach our dogs that certain behaviors make “good things” (reinforcers) happen, so our dogs learn to offer those behaviors in order to make good stuff happen.
Food is what we call a primary reinforcer, meaning it has innate value to the dog. Dogs don’t have to learn to like food; they are born looking for their mother’s milk. A scratch under the chin feels good – it has innate value – so that’s another primary reinforcer.
Other non-food reinforcers for dogs include: toys, sniffing, going on a walk or a car ride, or playing a game.
Verbal praise, however, is a secondary reinforcer; it takes on value through its association with a primary reinforcer such as food treats, excitement, and scratches under the chin. Toys, too, are secondary reinforcers; they take on value through their association with the predatory chase response. (Doubt this? Have you never met a dog who was initially mystified and uninterested in toys, but learned to play with them over time?)
How to do positive reinforcement dog training without treats
Nova will do anything for a ball. Sit? Sure.
Lie down? No problem.
Good dog! Okay, here you go!
Nova: “I have it now! So long, sucker!” She trots across the field for a private romp with the toy.
Oh man! Jessie has another ball! Abandoning the first ball, Nova responds to Jessie’s recall cue. The opportunity to chase a thrown ball is more reinforcing for Nova than the ball alone.
If you want to (or have to) make use of reinforcers other than food in your training, start by making a list of all the other things your dog loves. Here are some potential non-food reinforcers:
Tennis balls, or balls with a pleasing squishy texture
Squeaky toys
Playing tug
Playing “chase me” games
Going for a ride in the car (a chief pleasure for some dogs, aversive for others; know your dog!)
Leash walks
Off-leash hikes
Swimming (again, it’s important to know your dog; some hate water!)
Sniffing
Performing a favorite trick for an appreciative audience
For each item on this list, write down how you might be able to use that as a reinforcer in your training program. Some are easier than others. Here are some examples:
Use sniffing to reinforce your dog’s polite leash walking. Have your dog walk politely with you for a reasonable stretch (short enough that she can succeed!), then give her a release cue and say, “Go sniff!” (This works especially well at first if you give her the “Go sniff” cue when you know you are near something that she would like to sniff.)
Use tug to reinforce your dog’s “Stay.” Have your dog stay for whatever length of time she is able (set her up to succeed!), return to your dog, mark her for staying, give your release cue, then invite her to tug.
Remember to pause various lengths of time before your release cue, so she doesn’t start anticipating the release. You can even remind her to stay, hold up the tug, put it behind your back and hold it up again, several times, so the mere sight of the tug toy doesn’t become the cue to release from the stay. This, by the way, is a great impulse-control exercise.
Use a squeaky toy to lure and reinforce sits and downs. To lure a sit, hold the toy over your dog’s head the way you would a treat, and when she sits, squeak and toss the toy. To lure a down, slowly move the toy toward the ground and, when she lies down, squeak and toss. If that doesn’t work, move the toy under your knee or a stool, so she lies down to crawl after the toy. When she does, squeak and toss.
Use a tennis ball to reinforce your dog’s recall. She comes when you call, you mark her for coming, and then throw the ball for her to chase. If she’s one of those who won’t bring it back, have several balls within reach so you can call her back and toss the next ball when she comes. If you want her to sit in front of you as part of your recall, wait for her to sit before you mark and throw.
Now take your own list of reinforcers and write down scenarios that incorporate them into your training program. You will likely find some reinforcers that are impractical for training (say, the dog who loves to roll in deer poop), but you should end up with a treasure trove of possibilities!
If there are secondary reinforcers you would like to use that your dog isn’t already enthusiastic about, you can “charge” them by associating with something your dog already loves. If you want your dog to be happier about your verbal praise, repeatedly praise her and then throw her beloved ball, so she begins to associate praise with the joy of chasing a squeaky ball. If she’s not crazy about car rides, start taking short car rides that always end up at someplace wonderful (such as the swimming hole, if she loves swimming).
You get the idea. Whether your dog won’t take or can’t have treats, if you look for and create a good long list of other high-value options, you will always be prepared to reinforce your dog for appropriate and desired behaviors. She will love you even more for that.
Montana author Kathryn Dunning enjoys winter adventures with her dogs, who are also game to explore and play - even in sub-zero temperatures. But precautions must be taken to protect the dogs' paws.
The sky was a brilliant blue, with glimmers of sparkling snow flashingacross the path ahead as a light breeze blew it into the air, adding a pinch of magic to the scene. The temp hovered around a lovely 25°F (-3°C), and the only sound heard for miles was the swish of my skis combined with the heavy breathing of happy dogs with tongues lolling. We were running out of light, so I peeled off our scheduled route and zipped up a hill, a quicker, albeit steeper, way home.
As we climbed, I noticed my Border Collie pause briefly and look at his feet, but he kept going. I made a mental note to check his paws when we got home. We turned the corner, began our descent, and joyfully charged downhill.
Then, he stopped – suddenly – and started frantically biting at his feet. I kicked my way out of my ski bindings so I could reach him and help him with what I (correctly) guessed was bedeviling him: Snow had stuck to the hair between his paw pads, and icy balls had formed and expanded between his pads, causing his toes to splay uncomfortably. I felt terrible. In my enthusiasm to get out into this beautiful day, I failed to check the length of the fur on his feet before we left and he paid the price for my oversight.
Had I attended to this winter dog husbandry chore before we hit the trail, our outing would have been near perfect; the snowy, cold, but clear conditions were perfect for my athletic canine sidekick, who is well habituated to our chilly Montana winters.
THE BASICS OF WINTER PAW MAINTENANCE
John Wright raises and trains Springer Spaniels in Bozeman, Montana – and also takes beautiful photos of his dogs. Frequent nail-trimming, he says, is key to healthy paws in winter. Nails split and break more readily in winter – especially if they are too long.
But snow, ice, and cold aren’t the only foes our canine companions’ paws have to contend with in winter. In other parts of the world, there are other hazards that wreak havoc on the four-footed – including salt and other de-icing agents and persistently wet and/or muddy conditions – and a little regular maintenance goes a long way to keeping our friends up and running. Literally.
* Nail trimming. While many dog owners long to believe that time running on hard surfaces is sufficient to wear canine nails to an appropriate length, it’s just not so. No matter where you live, no matter what weather or surfaces your dogs are exposed to, regular nail trimming is vital to healthy paws.
John Wright, a trainer of champion Springer Spaniels in Bozeman, Montana, logs serious miles daily year-round with his dogs and knows all too well the importance of nail trimming. “Long, neglected nails are more likely to break or split in winter conditions with frozen ground or hard, slippery ice. A broken nail is a lame dog for a week or two,” he explains.
“Clip those nails! It’s quick and easy once you get the hang of it, it’s a 90-second gig for four paws,” Wright adds. Easy for someone with a lot of experience, perhaps less so for others. Nail trimming can be an anxious endeavor, which raises the anxiety for our canine companion receiving that care. Have you ever had your hair cut by someone who was unsure of what they were doing – or who actually nicked your ear with her scissors? That’s a chair everybody’s quick to jump out of!
An article in WDJ’s October issue (“Rotary Club”) discussed nail trimming techniques and tools. It may be additionally helpful to get an in-person tutorial on nail trimming from your favorite groomer or vet tech or whomever has the skills that instill ease and confidence in your dog. If you are like me, once you have the know-how you’ll wonder what you were so worried over in the first place!
I turn nail trimming into bonding time. At least once a month, my dogs get a relaxing turn at the (home) spa, complete with a pedi-pedi and a paw pad massage (more on this below).
* Hair trimming between pads and toes. As my experience on that otherwise perfect day illustrates, medium and long-haired dogs need to have the hair between their paw pads and toes kept short. This prevents the formation of snow and ice balls that can cause painful bruising and injury to tendons.
I prefer to do this myself, rather than go to a groomer, because it’s a quick and easy job with the right clippers. The best clippers for paws (around faces and ears too) are small, quiet, and cordless.
Many years and several pairs of clippers later, I discovered Cyrico cordless professional pet clippers and swear by them. Forget about trying to find an outlet in a spot where hair can conveniently fly; cordless trimmers allow you and your dog to be wherever you are most comfortable. And they hold their charge surprisingly well! (Here is a link to my favorites:tinyurl.com/WDJ-cordless-clippers.)
Whatever clippers you choose, it’s helpful if they are relatively quiet, helping to reduce noise and vibration, which can trigger anxiety in some dogs. Of course, even the quietest clippers still make noise, so I found it helpful to teach my dogs to associate a tasty treat (they highly recommend bacon-flavored Cheez Whiz) with the sound of clippers before they even touch the dog’s fur. It’s a tiny bit of effort that allows for a lifetime of calm clipping.
If the snow doesn’t fly where you live, but the rain is frequent, keeping the hair trimmed on your dog’s paws will reduce mud and crud that can accumulate between the dog’s toes (and track onto your floors), and it helps paws to dry properly. Excess water can create bacterial buildup between the toes, leading to itchiness, sores, and infections.
* Protect with paw balm. Salt and chemical deicers on sidewalks are great for reducing slips, but can cause paws to become irritated, and some can be dangerous if ingested. Applying a balm to paws prior to heading outdoors provides a nice buffer between the paw pads and the treated walkways.
The reigning standard balm for paw protection in winter (and summer!) is Musher’s Secret. It’s made from a blend of food-grade, organic waxes that form a semi-permeable shield on the pads, allowing perspiration to escape through the toes. It’s also non-toxic and non-allergenic.
While I find it to be a very useful product, its maker claims that Musher’s Secret will prevent balls of ice and snow from forming on a dog’s paws and in between their toes. In test after test on a variety of dogs, all medium and long-haired, Musher’s Secret has never prevented paw-snowballs for my dogs. Ever. This is not a deal-breaker, just a bit of an over-sell.
You will still have to keep paw hair trimmed. (If this just prompted groans, I assure you trimming is not that bad. In a winter season in Montana that lasts six months or more, I trim paw-fur three or four times and it takes five minutes or less per dog. It’s really not that bad!)
Here’s another winter hazard for our dogs’ paws: those huge swings in temperature and humidity as you travel indoors and out. These are absolutely fabulous conditions for drying out and cracking paw pads– your hands likely suffer the same fate in winter! I personally want one balm to rule them all, protecting and treating dog paws and mine too, so I make my own (see my recipe on page 15). I add essential oils to enhance the spa experience!
Ruffwear’s Polar Trex Winter Dog Boots
* Boots. There comes a time when winter conditions will make boots your best friend’s best friends.
Dogs have varying sensitivity to cold, but by -10°F (-23°C), you start to see all dogs holding up paws, sometimes trying to simultaneously lift three or four paws off the cold surface – it’s quite a sight to behold!
Older dogs, especially, don’t thermoregulate as well and their feet become increasingly sensitive to cold. Boots can make a huge difference for them, allowing them to comfortably get out and enjoy winter. Dogs with short or thin coats need extra protection, too.
However, if your dog has never worn boots and you suddenly toss them on, prepare for a high-stepping protest march complete with bucking and kicking. Boots take some getting used to.
You’ll have to spend some time introducing them to your dog. Putting them on and then doing something fun right away distracts them from this new, very awkward accessory. Several short sessions will start to ease a dog toward boot-happiness.
A good fit is critical for your dog’s comfort, although it can be challenging to find just the right size; every manufacturer’s sizing varies slightly. When in doubt, order products in the two closest sizes and try them on indoors at home. Don’t try to “make do” with a close fit; you’ll just end up hurting your dog and souring him to future attempts with better-fitting boots.
How should you identify good boot candidates? Look for:
• Durability. Look for quality material without excessive bulk.
• Flexibility and comfort. Dog boots need to be supple and flexible, especially at the dogs’ wrists and ankles. Dismiss the ones that are stiff throughout, rising high on the leg, with a lot of straps to keep the boot in place, which can hinder movement and do more damage to a foot than the elements!
• Good workmanship. Seams, zippers, and patches of hook-and-loop material (such as Velcro) should be minimal, and nothing should feel rough on the inside of the boot. Anything that protrudes on the inside of the boot can cause sores on the dog’s foot or leg.
• Visibility. The brighter the boots, the more likely you will find them after your dog manages to lose one or more.
I’ve tried many models from a number of companies, but I find myself going back to the same two companies again and again.
Ruffwear (ruffwear.com) is great about helping dog owners find the right boot and fit for their dogs’ needs. Most of their boots are a bit technical; figuring out how to get them on and worn comfortably can take some work, but they’re worth it.
Hurtta (hurtta.com) also makes great boots. Their products are easier to put on the dogs and tend to be comfortable straight out of the box with minimal fuss.
Once your dog is accustomed to his boots, don’t tune out; you need to stay alert to any sign of discomfort. If a boot slips or twists, it won’t take long for an errant seam to rub a paw raw. Check the fit periodically when you’re out to prevent these sorts of unfortunate boot-mishaps. Few things can ruin an outing faster than a boot rubbing the wrong way.
Homemade Paw Balm
Yields six 1-oz jars
You’ll need:
•Small pot and glass bowl or double broiler
•2 oz olive oil
•2 oz coconut oil
•1 oz shea butter
•4 tsp beeswax
•Optional scent: Use only therapeutic-quality essential oils to meet your personal scent preference. My favorite combination is 3 drops each oflavender, mandarin, and chamomile essential oils.
•Also optional: 1⁄4 tsp vitamin E oil as a preservative
1. Pour an inch or two of water into the bottom of a double boiler, or set a glass measuring cup into a pot of water so that the glass bottom is submerged and the top is exposed. Bring the water to a simmer.
2. Add coconut oil, olive oil, and shea butter to the glass cup or the top of the double boiler.
3. As the mixture warms and melts together, add the beeswax. When the beeswax begins to float to the top, stir the mixture continuously.
5. Set out six 1-oz jars and add the essential oils (and optional vitamin E for increased shelf life) to each jar.
6. Pour the melted base into the jars. Stir lightly (a chopstick works well for this) to mix the essential oil and vitamin E into the base.
7. Cover with breathable material (e.g., cheese cloth) and cool until they harden.
Enjoy for one long, cold winter (longer if you add the vitamin E).
Tether your dog in locations where he is safely out of household traffic and can't get tangled in anything. Give him a comfy mat or bed and a food-stuffed toy or chewy.
I’ve long been a proponent of the appropriate, judicious use of tethers for dog training and management. This doesn’t mean tying up your dog in the yard all day while you’re at work, or for hours while you’re grocery shopping; it means short-term restraint under the direct supervision of a responsible human. Proper use of tethers can be a lifesaver in your dog’s training and management program.
You can purchase ready-made tethers (my favorites are from pettethers.com)or make them yourself out of sturdy, good-quality materials. While some people just tether with their dog’s leash, I don’t recommend this (except for short-term emergency tethering), as your dog can chew through a leash. A nylon-coated cable tether with sturdy clips on both ends can be attached to an eye-bolt screwed into a solid wall beam.
We recommend tethering only with a plastic-coated cable, which resists tangling and can’t be chewed.
Alternatively, if you clip the tether to an eye-bolt screwed into a block of wood, you can then slide the tether under a door and close it; the door will hold the tether in place (as seen in the photo above).
You can also use the Pet n’ Place anchoring system to set up a portable tether outdoors and/or when you are traveling. This product is suggested for dogs who are less than 60 pounds; if your dog weighs more, use two!
APPLICATIONS
There are a multitude of ways a tether can enhance your life with your dog, including:
* Housetraining. Reduce your not-yet-housetrained dog’s crate confinement by tethering instead of crating. It’s easy keep him with you as you move around the house, and he will still be inhibited from soiling his immediate tether space.
* Chewing. Rather than crating to supervise his puppy/adolescent predilection to chew everything he can get his teeth on, tether in chew-proofed locations so he can still accompany you around the house.
* Polite greeting. Tether your dog while you repeatedly approach to teach him to sit politely to greet people. You can also tether him while you greet visitors to your home, and then instruct your guests on how to greet him in order to reinforce polite greetings. For example, “When all four of the dog’sfeet are on the floor, you can pet him. But if he jumps up, just step back out of range.”
* Present yet managed. Your dog may be social – perhaps too social. If he’s inclined to sit in everyone’s lap and not all your guests appreciate close encounters of the canine kind, you can tether him, rather than shut him away in a back room. He still gets to enjoy the company but can’t pester people. Again, coach your visitors that if they want to approach him, he needs to offer a polite sit in order to be greeted.
* Counter-surfing. In the kitchen, this is a must-do while you work to modify his counter-surfing behavior! (See “Useful Matters/Mat Training Tips,” WDJ January 2020 and “Counter Productive,” July 2020.)
*Training. Use a tether when you need your dog to stay in one place during a training or behavior modification session, but his stay is not yet solid, for example, while playing “Nose Games,” etc. (see “Everyone Nose That/Understanding Your Dog’s Nose,” September 2019).
* Other animal companions. If your dog is an attention hog, and every time your other dog comes up for some petting, he pushes her away and demands that you pet him instead, use his tether to ensure that she gets equal petting time. If your dog chases the cat out of the living room every time she tries to come in for a lap-visit, tether him and do counter-conditioning for the presence of the cat while also giving your feline family member some safe living room time.
* Restricted activity. If your dog is on the dreaded “restricted activity,” and if he will stay calm on a tether, tethering can be an alternative to crating.
* Feeding. Perhaps one of your dogs tends to gobble his food so he can go scavenge your other dogs’ bowls before they are done. You can tether your gobbler at his feeding station so you don’t have to constantly play traffic cop.
* Human mealtime. If your dog has learned the fine art of begging at the table, you can enhance your own dining experience by tethering him nearby, far enough away to prevent him from bugging you. He gets to be part of the family at mealtime but learns to mind his manners.
The tether can be a great tool when used properly and can be instrumental in helping your dog stay in your lifelong loving home rather than be rehomed, or even euthanized. Value it, and use it with care.
Tether Do's & Don'ts
The tether isn’t for every dog, nor every restraint situation. Here are some things to keep in mind if you use a tether with your dog:
Do these things when tethering:
✓ Take the time to introduce your dog to his tether gradually, with treats, so he has a positive association with it. This is especially important if he is sound-sensitive, as the tether clips can make a clanking noise, or if he has prior negative experiences with being chained or tethered.
✓ If your dog has any tendency to pull hard/yank on his tether, attach the tether to the back clip of a harness to avoid potential damage to his neck.
✓ Instruct your guests on how to greet your dog properly when he’s tethered, and provide them with treats so they can reinforce him properly when he sits.
✓ Provide constant supervision for your tethered dog so he can’t become tangled and injure himself.
✓ Provide your dog with a food-stuffed toy or other chewie when appropriate (i.e., if you are tethering during your meals) to help him settle and relax on his tether. (You can tether a stuffed Kong to his tether attachment so it doesn’t roll out of his reach.)
Don’t do these things when tethering:
✓ Don’t use a tether if your dog is even mildly frightened or wary of it, unless you do ample conditioning first to convince him that it is wonderful.
✓ Don’t use the tether as punishment. It’s okay to use it as a calming time-out, but it should not be associated with any reprimands or coercive handling.
✓ Don’t leave your dog tethered and unattended. He can become tangled and injure himself.
✓ Don’t tether your dog where he can be harassed by other dogs or humans.
✓ Don’t tether your dog with a flat collar if he tends to pull hard on his tether, and never tether your dog on a choke chain or other collar that tightens. (They are called “choke chains” for a reason!)
✓ Don’t tether your timid dog where unfamiliar humans can approach him. If he must be tethered when humans are present, tether him at a distance where he can feel safer and you can still keep an eye on him, and surround him with exercise pens so no one can approach past his threshold distance. If he’s significantly fearful, do not tether him, ever, where unfamiliar humans might approach. Instead, put him in a safe room away from the action, inaccessible to visitors.
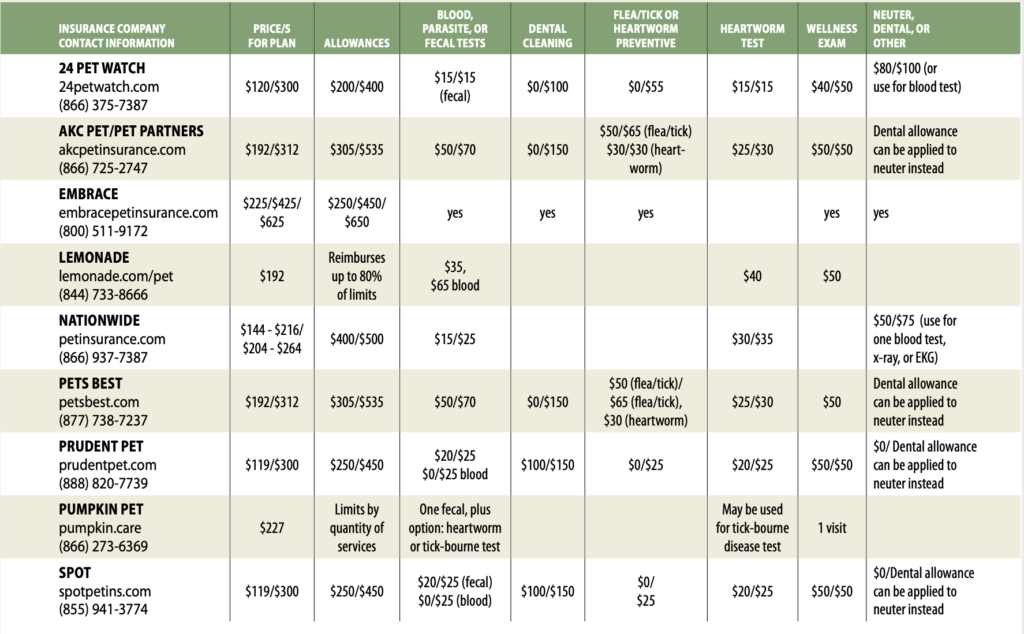
Wellness visits are not covered by most "major medical" pet insurance plans. If you'd like an entire year to spread out the cost of routine care (a well-pet checkup with a blood test and perhaps a vaccination, heart worm test, and a prescription for a heart worm preventative), adding a wellness rider to your dog's major medical plan might work well for you.
At the close of 2019, 2.82 million pets had health insurance, according to the North American Pet Health Insurance Association. Over the past five years, the industry has grown 22.1% annually on average. That outstanding growth rate is big news.
But pet insurance isn’t news to our readers. We’ve discussed the topic in depth twice over the past five years, in the September 2015 and March 2018 issues. And little has changed since those articles were published except for one thing: the increased number of companies offering wellness riders – optional insurance policy provisions that add benefits to or amend the terms of a basic policy.
“WELLNESS PLANS” ARE NOT HEALTH INSURANCE
Traditional pet health insurance plans help owners pay for the costs of diagnosis and treatment of unexpected and/or catastrophic injuries or illnesses; they don’t usually cover the cost of routine well-pet exams.
Historically, pet insurance companies have offered “wellness” or “preventive” coverage as an add-on to a traditional pet health insurance policy. These are often marketed as incentive programs that will motivate us to make annual or semi-annual well-pet visits. If you’ve paid for a well-pet visit already in the form of a wellness rider that will reimburse you for that visit, you are more likely to follow through and get your dog in to see the vet! The twist is: If you don’t go, you don’t get reimbursed!
We’re all for well-pet visits. Dogs who are seen by their veterinarians regularly are most likely to have any problems with their health detected in the earliest stages, when treatments are most effective. Any tool that encourages owners to schedule these visits can literally save dogs’ lives. There’s a big catch, though: Despite the fact that the insurance companies market wellness riders as a way that owners can reduce and plan for the cost of routine veterinary care, these plans won’t necessarily save you money. They can do so – but you have to be extremely organized and knowledgeable about what routine care your dog will benefit from in the year ahead in order to realize savings from their purchase.
HELPING KEEP YOUR DOG’S HEALTHCARE ON TRACK
To repeat: Classic wellness plans essentially act like a financial incentive program that encourages the pursuit of routine veterinary examinations by reimbursing the insured pet’s owner for a set of pre-selected benefits, such as a well-pet visit, a screening blood test, vaccinations, heartworm testing, etc.
For example, a wellness rider may cover the cost of an annual heartworm test and reduce the cost of monthly heartworm preventative medications. The routine administration of the preventative keeps your dog free of heartworms – and reduces the chance you will file a claim for a dog who needs treatment for heartworm disease.
As another example, some companies’ wellness plans reimburse owners for a significant part of the cost of an annual dental cleaning. In small dogs, many of whom suffer periodontal problems that result in tooth loss, annual cleanings can help a little dog avoid losing 20 teeth in a $3,000 surgery – a win for everyone involved.
WHAT’S THE CATCH?
Again, these wellness riders are offered as adjunct to, not replacements for, your dog’s health insurance, which is what does help cover the cost of unexpected trips to the vet for injury or illness. Think of wellness plans, instead, as a pro-rated trip or two to the vet, where the cost is spread across an entire year, which can help ensure it’s in your monthly budget.
As such, the potential reimbursements offered by the wellness plans are strictly limited in value. A plan that costs you $30 per month, for a total cost to you of $360 per year, might have an annual allowance of $400. Yes, the potential savings for that year is only $40 – and you will save that money only if you use every penny of the annual allowance by booking all of those wellness benefits. You could actually lose money on the plan if you fail to schedule and bring your dog in to your vet for the services you’ve paid for.
Honestly, it’s a bit like a casino: Unless you are a very savvy consumer, the odds favor the insurance company. It’s far more likely that the average dog owner will pay more for a wellness “plan” than they will receive as reimbursements for services their dogs enjoyed. You can get more value out of a wellness plan that you pay for in a monthly premium, but again, you have to be organized. You have to thoroughly research the plan ahead of time, making sure it will pay for (or significantly reduce the cost of) all the routine healthcare you plan to obtain for your dog – and then make sure you get that care. If you aren’t that disciplined, you may well lose money on these plans.
Comparing Wellness Plans Offered by Health Insurers
The table below lists only some of the many companies offering wellness riders to their health insurance plans and only some of the benefits the plans include. The health insurance companies don’t make it easy to compare their products with those of their competitors, but we’ve tried to simply illustrate how different the available plans are.
The prices listed here are the amounts we found for wellness plans for a 2-year-old, small, mixed breed dog. As we built this table, we noticed that prices and allowances change frequently; these are accurate as of 10/1/20.
Some companies offer more than one benefit level; we’ve used a slash symbol ( / ) to indicate the prices, allowances, and benefit levels of each tier of the plans offered.
The largest benefit offered by many companies in their wellness plans is a reimbursement that can be used either for a spay/neuter surgery, dental cleaning, or other major expense. Our guess is that this is done because a dog may need spay/neuter surgery as a younger dog or a dental as an older dog, but rarely both in the same year. We showed those major benefits in the last column.
COVERAGE WILL VARY
The wellness plans offered by pet health insurance companies vary widely. Some give you a ton of options; some lock you into a specific and limited set of veterinary services that qualify for reimbursement.
Some of the plans offer an extensive list of preventive options that you can use in their wellness plans. Embrace Pet Insurance, for example, includes Reiki, massage therapy, anal gland expressing, wearable pet activity monitors, acupuncture, and even medicated shampoos in the list of services that the plan will reimburse you for. Other plans, like Pumpkin Pet Insurance’s “Preventive Essentials Package,” focus on preventive basics with one well-pet veterinary visit, one fecal test, one test for a vector-borne illness test (such as Lyme disease), and two vaccinations.
The difference is reflected in the cost. A wellness rider from Embrace for a small 2-year-old dog would cost $35 a month (a total cost of $420 for the year) with a $450 allowance. It offers the widest range of coverage choices we found and doesn’t dictate how much you can spend on each item. You could choose to spend the entire $450 allowance on acupuncture therapy, if you wanted – and you could do it all the first month of coverage, if you wished, but you still would be required to pay the monthly premiums for both wellness and health insurance for the full year.
Most riders we examined used monetary limits for their wellness coverage by individual items. For example, AKC/Pet Partners will reimburse you for a maximum of $50 or $65 (depending upon the level you choose) for flea and tick prevention. The actual the cost of a year’s worth of spot-on flea treatment for a small dog is more than that – depending on the product used, it may cost as much as $120. In cases such as this, the plan simply helps defray the cost of caring for your dog; it won’t cover the entire cost.
Other plans cover a set quantity of specific services, such as the Pumpkin Pet package described above. The cost for this package for our hypothetical 2-year-old small dog would be $19 per month, for a total cost of $228.
That sounds great – mostly because, at many clinics, the cost of all that likely exceeds $228, so Pumpkin Pet’s reimbursement to you for all that should mean that you saved money. But you need to read the insurer’s customer agreement carefully to see if they have limits on how much they will reimburse you for that one veterinary wellness visit.
Another Option: Wellness Packages Offered By Veterinary Practices
Many veterinarians and veterinary companies, like the 1,000-clinic Banfield Pet Hospital, have designed “wellness packages” for their clients. The benefit to you, as with any wellness coverage, is that it helps to defray the cost of the preventive measures your dog needs to be healthy. The benefit to them is that it pretty much binds you to their veterinary clinic for the year.
These plans are prepaid preventive options that don’t require you to also purchase an accident/illness policy. They can be extremely helpful to those on a budget because, when working directly with your own clinic, you usually don’t have to pay the money up front and then be reimbursed. You just pay your monthly premium, and your dog gets the preventive care he needs.
THE RIGHT RIDER
Not all screening tests and preventive procedures are necessary. Ask your veterinarian for recommendations regarding preventive care and health screens, based on your dog’s age, activity, and predominant breed.
Keep in mind that most of these riders are offered in combination with your accident/illness coverage. Because that part of your policy is your primary concern, the first thing you need to do is decide which insurer offers what you need for your dog. For more information about choosing a major medical policy, see “Rest Insured,” WDJ March 2018. To recap that article briefly: We advise that you choose an accident/illness policy without monetary or treatment policy limits and that you make sure that the actual fees on your veterinary invoice are used to determine reimbursement (as opposed to a “fee schedule”).
Also important: Read the policy in full to ensure that any exclusions will not be a problem for you – and there are usually a lot of exclusions. For example, if you have a German Shepherd Dog, you’ll want to be sure hip dysplasia is covered. If you have a Papillon, look carefully at the dental coverage. Your veterinarian can offer an expert opinion to help you choose.
After you’ve chosen your dog’s “health” insurance, read the wellness rider in full before you sign. Sometimes, the broad-strokes description of a wellness plan leaves owners with a more generous impression of what they will get for their money than what is described in fine detail in the customer agreement.
And, finally, remember that you need to exhaust the available benefits of a wellness plan over the course of the policy year to make the policy worth having; the funds do not roll over from year to year. If you have a $450 allowance and you used only $300 of it, you will have lost $150 when the policy renews.
Cynthia Foley is a freelance writer and dog agility competitor in Warners, New York.
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.
This website uses cookies and other tracking technologies to offer you a better experience, personalize content and ads, and analyze our site traffic. Before proceeding, you agree to our Terms and that you’ve read our Privacy Policy. Update Settings
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.