A very small percentage of Cushing’s cases result from medical treatments for other conditions, such as the use of prednisone or other corticosteroid medications to control allergies, arthritis, or autoimmune conditions. This is called “iatrogenic” (doctor-caused) Cushing’s. In these cases, the Cushing’s is treated by gradual discontinuation of the corticosteroid drugs (if the drugs are withdrawn too quickly, an Addisonian crisis can result). Patients can take as long as three months to recover after corticosteroid drugs are stopped.
Also known as Alopecia X, pseudo-Cushing’s is identified by symmetrical alopecia (hair loss) on the trunk of the body, thighs, or neck, along with darkening of the skin where hair is lost. The coat’s color may change as well. The condition does not cause itching.
Pseudo-Cushing’s is seen in young dogs (ages 1 to 5) with plush coats, such as Pomeranians, Poodles, Samoyeds, Alaskan Malamutes, and Siberian Huskies. Pseudo-Cushing’s is thought to be a mild form of pituitary-dependent hyperadrenocorticism.
Dogs with this disorder may respond to castration, methyltestosterone, melatonin, growth hormone supplementation, or one of the drugs used to treat Cushing’s disease. One study showed that 90 percent of dogs with pseudo-Cushing’s treated with trilostane responded within eight weeks.
1. Don’t dismiss changes in your dog as normal aging. Your veterinarian may find an underlying, treatable cause.
2. Treatment for Cushing’s can improve quality of life for your dog. Don’t be afraid to try drugs when needed.
3. Watch closely for signs such as lack of appetite that may indicate drugs need to be stopped or dosage adjusted.
4. lf your dog has all the signs of Cushing’s but tests are negative, consider atypical Cushing’s or adrenal exhaustion as a possible cause.
Sometimes life-threatening illnesses develop so slowly that no one pays much attention. An older dog who’s always thirsty drinks huge quantities of water. He’s hungrier than usual and has developed a thin coat and pot belly. He pants all the time, and now his hind legs are losing muscle tone and getting weak. Many owners dismiss these as normal signs of aging, but they are classic symptoms of Cushing’s disease, which affects an estimated 100,000 dogs in the U.S. every year.
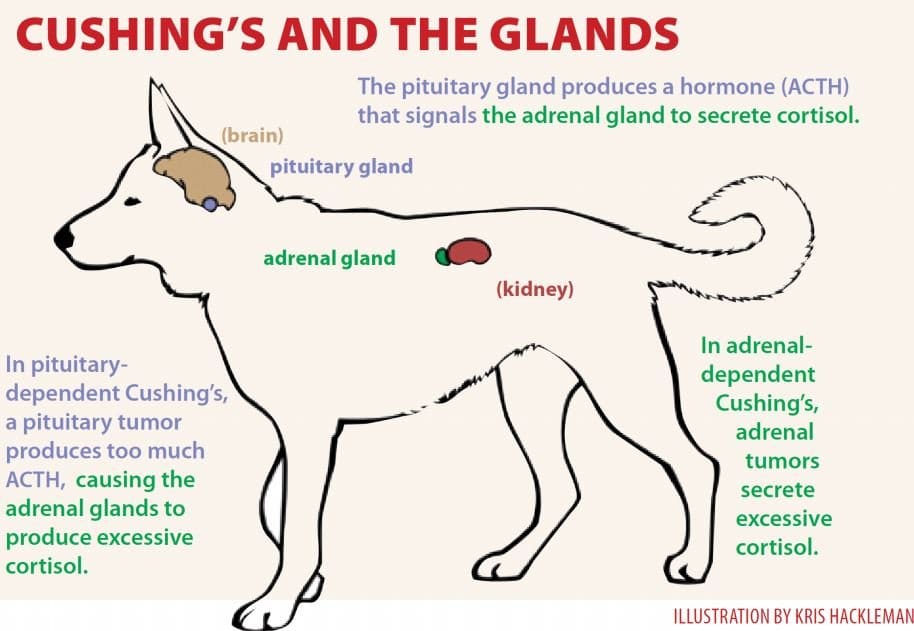
Also known as hyperadrenocorticism, Cushing’s is the opposite of Addison’s disease. Both illnesses involve the adrenal glands, which produce cortisol – a stress hormone that helps prepare a dog for fight or flight by breaking down muscle and fat to convert into glucose. While Addison’s disease results from insufficient cortisol, Cushing’s disease results from too much – and prolonged exposure to cortisol can have negative effects on the entire body. Cushing’s puts dogs at increased risk for diabetes, pancreatitis, calcium oxalate bladder stones, pulmonary thromboembolism, hypertension (high blood pressure), urinary tract infections, protein-losing kidney disease, hair loss, skin problems, and congestive heart failure.
Cushing’s disease affects primarily middle-aged and older dogs. The majority (about 85 percent) of Cushing’s disease cases are caused by tumors of the pituitary gland; these are usually benign (adenomas). About 15 percent of Cushing’s cases are caused by tumors of the adrenal gland; about half of these adrenal tumors are benign and about half are malignant (carcinomas).
In pituitary-dependent hyperadrenocorticism (PDH), tumors cause the pituitary gland to overproduce adrenocorticotropic hormone (ACTH), which signals the adrenal glands to release cortisol. The average age at diagnosis with PDH is 10 years, and the most commonly affected breeds are Poodles, Dachshunds, Beagles, German Shepherds, Boxers, Boston Terriers, Labrador Retrievers, and terriers, with 75 percent of patients weighing less than 44 pounds.
With adrenal-dependent Cushing’s, the adrenal tumor itself secretes excessive cortisol. The average age for diagnosis with adrenal tumors is 11 years, with Poodles, German Shepherds, Dachshunds, Labrador Retrievers, and terriers predominating. About half of all cases occur in dogs weighing more than 44 pounds, and females may be more commonly affected.
Kris Hackleman
Pituitary Cushing’s Disease in Dogs
Girl, a Miniature Schnauzer, has lived with Cindy Bright of Indiana, Pennsylvania, since her first owner passed away in 2006. Girl is famous for eating anything (including dehydrated or living toads); at 27 pounds, she was seriously overweight.
By February 2008, Girl’s symptoms included excessive thirst and urination, overeating, urinary incontinence, and occasional hyperexcitement or aggression. She was diagnosed with PDH and was given Vetoryl (trilostane), a drug that was not approved in the U.S. until 2009 for the treatment of both pituitary- and adrenal-dependent Cushing’s, but which has been used in the U.K. since 2001. Bright imported the drug from the U.K. (something that could be accomplished with a prescription and by filling out a form to obtain permission from the FDA).
Today Girl is doing well, and her weight is a normal 19 pounds. Her occasional health setbacks tend to follow dietary indiscretions, such as her consumption of a 6-pack of English muffins that someone set outside the basement freezer and her indulgence in wild rabbit droppings, which Bright describes as Girl’s “caviar.” Girl suffered a serious bout of pancreatitis in 2010. “Life is like walking the tightrope,” Bright says. “One slip and it’s difficult to get everything back on course.”
Like Girl, all dogs with Cushing’s disease require careful monitoring. Depending on the drug used to control symptoms, even minor changes in condition or behavior can signal major problems, and conscientious caregivers keep a close eye on anything that seems unusual or different.
In Springfield, Vermont, Kathy Mason’s Beagle, Chance, was diagnosed with PDH at 8 years old. He was treated with Anipryl, which was not effective, and then switched to Lysodren (mitotane). “After about two years of good bloodwork,” says Mason, “Chance went into an Addisonian crisis. We thought we were going to lose him, but he survived and stayed Addisonian for the rest of his life. It was so much easier to treat. He passed away in January, five years post diagnosis, at the age of 14 years old.”
While most pituitary tumors are microscopic, 10 to 20 percent are larger than 10 millimeters (3/8 inch) in diameter. Called macrotumors or macroadenomas, almost all of these pituitary tumors are benign, but about half are large enough to compress the brain and cause neurological symptoms such as listlessness, poor appetite, confusion, walking in circles, or seizures. Most dogs are diagnosed with Cushing’s at least six months before neurological symptoms develop. Breeds with short noses, such as Boxers and Pugs, tend to have the largest pituitary tumors.
Most dogs with pituitary tumors are treated with medication because their tumors are considered inoperable. However, a rather new surgical technique allows some tumors to be removed.
Another option for large pituitary tumors is radiation therapy, which is expensive ($3,000 to $5,000 in the Los Angeles area) and can have adverse side effects such as skin and hair loss, hearing loss, or problems with tear production in the eyes. Although successful in 70 percent of cases, further treatment for Cushing’s is usually required, and tumors treated with radiation are likely to recur. Survival time is not increased if neurological problems are severe.
Adrenal Cushing’s Disease
hree years ago Maggie, a 12-year-old black Labrador Retriever/hound-mix in Atlanta, Georgia, developed a voracious appetite, drank incredibly large amounts of water, and began raiding the trash. Her owner, Kristin Boggs, took Maggie to their veterinarian, who suspected Cushing’s. “Usually Cushing’s is pituitary-based,” she says, “but instead of assuming this, my vet ordered an ultrasound test. He had once before seen a case of Cushing’s that was caused by an adrenal tumor. Sure enough, Maggie had a large tumor on her adrenal gland.”
The solution was to remove the entire gland. Maggie’s surgery took place at a special internal medicine veterinary clinic, where a post-surgical nurse attended her through the night.
“Maggie came through with flying colors, despite an incision almost the full length of her belly,” says Boggs. “She’s a tough old girl. Thankfully the tumor was benign. After a few weeks of medication to balance her cortisol levels, she was back to normal.”
In Toledo, Ohio, Linda Boyle’s Springer Spaniel, Cody, was diagnosed with Cushing’s disease at age 11 after developing a ravenous appetite and gaining weight. Cody’s ultrasound exam revealed tumors on both adrenal glands.
“A bilateral adrenalectomy is very risky,” says Boyle, “but it worked well for Cody. He became an Addison’s dog because his body no longer produced any cortisol at all, but he lived another two years with good quality of life before passing away from what we believe was pneumonia.”
Because Cushing’s patients tend to have high blood pressure and poor healing ability, several months of medical therapy may be needed to strengthen the patient prior to surgery. After surgery, prednisone or other corticosteroids may be required for a few months until the dog’s ability to produce cortisol recovers, and some dogs may need mineralocorticoid replacement as well.
In a survey of 63 dogs who had surgery, 4 (6 percent) had inoperable tumors and were euthanized; 18 (29 percent) died during surgery or soon after because of complications; and the average post-surgical life span for the remaining 41 dogs was 46 months.
As this article goes to press, Maggie’s Cushing’s symptoms have returned, caused by a new tumor on her remaining adrenal gland. “I can’t believe this has happened to us again,” says Boggs. “It’s an exact repeat of what we went through three years ago. We don’t know if the tumor is malignant or benign, as we don’t feel extensive surgery at her age (15 ½) is reasonable. My vet and I have decided to treat her with trilostane and see how she does. My priority now is that she is happy and comfortable.”
Diagnosing Cushing’s Disease in Dogs
Cushing’s disease isn’t always easy to diagnose. Routine test results that can point toward Cushing’s include:
High or very high alkaline phosphatase (ALP, ALKP, SAP). Although this is a “liver enzyme,” marked elevation is associated with cortisol. It does not indicate liver disease if other liver enzymes such as ALT (alanine aminotransferase) are normal.
Increased neutrophils and decreased lymphocytes (stress leukogram).
Elevated cholesterol and triglycerides due to abnormal fat mobilization.
Fasting hyperglycemia due to insulin resistance.
Liver enzymes may be mildly elevated.
Dilute urine (low specific gravity) due to excessive drinking.
Protein in urine (microalbuminuria or proteinuria).
X-rays may show an enlarged liver and occasionally calcium deposits in the skin (calcinosis cutis, which feel like rocks and cause itching).
Dogs with Cushing’s are prone to bladder, skin, and other infections due to the immunosuppressive effects of cortisol. About 20 percent of dogs with Cushing’s have an inapparent bladder infection, requiring a culture (not just urinalysis) to detect.
Confirming a Cushing’s diagnosis can be challenging, especially as false positives are common in dogs with nonadrenal illness. The following tests are commonly used:
Urine Cortisol:Creatinine Ratio (UCCR) is a screening test only. A negative result rules out Cushing’s, but anything that increases stress can cause a positive result, necessitating further testing. Use urine samples caught at home for this test so that the stress of a vet visit doesn’t influence the results.
Low Dose Dexamethasone Suppression (LDDS), considered the most accurate for diagnosing Cushing’s, takes eight hours in the hospital. A baseline blood cortisol level is measured, then a tiny dose of dexamethasone (corticosteroid) is injected. In a normal dog, blood cortisol levels drop after eight hours. Blood samples are sometimes checked after four hours, as this can help classify the form of Cushing’s. About 95 percent of dogs with Cushing’s test positive, but false positives are also common, and the more severe a nonadrenal illness, the more likely a false positive result. This test is preferred if an adrenal tumor is suspected.
ACTH Stimulation: No longer recommended for diagnosis, as its sensitivity is poor, its cost is high, and it cannot differentiate between pituitary and adrenal forms. This test is more specific than LDDS, however, meaning that strongly positive results definitely indicate Cushing’s disease, and false positives are unusual, but false negatives are common.
This test is useful for monitoring treatment, and it is the only test that can be used for dogs currently being treated with corticosteroids. A low-normal or blunted response indicates iatrogenic Cushing’s (see sidebar, facing page). This may be the preferred test if symptoms are mild, for it is better to miss the diagnosis than get a false positive.
Test results must be considered in combination with symptoms. A dog with at least three of the typical signs plus a positive test is considered to have Cushing’s, but a dog with no signs but maybe high ALP and a positive test may not, in which case it’s best to take a wait-and-see approach. If signs are present but test results are negative, consider retesting in three to six months or test for atypical Cushing’s.
Different Types of Cushing’s Disease
Classifying the type of Cushing’s disease as pituitary or adrenal helps determine which treatment is best. The endogenous ACTH level is felt by many to be the most accurate method of identifying the type of Cushing’s, but this test is difficult to run, as serum must remain frozen during transport to the lab. Dogs with pituitary tumors have high ACTH levels, while those with adrenal tumors will have low or no measurable ACTH.
LDDS may be used for classification when a 4-hour sample is drawn. If the 8-hour sample is > 30 nmol/L and the 4-hour sample is < 30, or both are less than half of the baseline sample, the pituitary form is likely.
The high dose dexamethasone suppression (HDDS) test is similar to LDDS, but a high dose of dexamethasone is used. This test is done only on dogs already known to have Cushing’s. Dogs with a pituitary tumor will show suppression in circulating cortisol levels 75 percent of the time, but those with adrenal tumors never show suppression.
Adrenal tumors can be seen on ultrasound 30 to 50 percent of the time. An adrenal tumor is suspected whenever one adrenal gland is observed to be enlarged while the other is not visible. If they have not spread, adrenal tumors should be removed, if possible, but surgery is difficult and usually requires a specialist.
Two normal or large adrenal glands indicate the pituitary form of Cushing’s, although enlarged adrenal glands are also often seen in cases of nonadrenal disease due to the chronic stress of the illness. An MRI or CT scan can detect pituitary tumors and determine their size. Two-thirds of dogs with tumors greater than 10 millimeters initially will develop neurological signs and may benefit from immediate radiation therapy, even before signs are seen.
Medical Treatment for Cushing’s Disease in Dogs
The best treatment for Cushing’s disease depends on the severity of symptoms, type of Cushing’s, risk of adverse effects, and cost factors. Medical therapy is used to control clinical signs, but it does not cure the disease. It is not likely to prolong life but does improve the dog’s quality of life. Not treating is also a viable option, particularly if symptoms are minimal. In this case, complementary care may be especially useful.
If the dog suffers from a concurrent medical condition, it is important to treat and stabilize that illness if possible before treating for Cushing’s. Treatment for dogs with concurrent nonadrenal illness, such as diabetes, is complex and beyond the scope of this article.
Mitotane
Mitotane (Lysodren®), which is used for both pituitary and adrenal Cushing’s, was the only treatment available until recent years. Mitotane is convenient and relatively inexpensive, but it has potentially severe side effects. A chemotherapy drug, it works by selectively eroding the two inner layers of the adrenal cortex that produce cortisol while tending to preserve the outer layer that makes aldosterone. If too much is eroded, the result is a cortisol deficiency.
About 30 percent of dogs treated with mitotane develop short-term reactions. If this happens, mitotane is discontinued and the dog is treated with prednisone until the adrenal glands recover. The destruction may be permanent, requiring treatment for atypical (or sometimes typical) Addison’s. Mitotane’s risk of a permanent or life-threatening Addisonian reaction is considered 2 to 5 percent.
Mitotane is given once or twice a day during the “induction” phase, during which adrenal erosion is induced. The drug must be given with food or it will not be absorbed. Mitotane should not be used for dogs with a poor appetite; inappetence indicates that something else is going on that must be diagnosed and addressed prior to beginning Cushing’s therapy.
During the induction phase, caregivers should notify their veterinarians as soon as their dog experiences any appetite reduction, decrease in water consumption, diarrhea, vomiting, lethargy, or listlessness. It is important to watch for these signs starting around the third day of treatment. These symptoms indicate that the end of the induction has been reached and it’s time for an ACTH stimulation test.
The induction time is variable, usually between 7 and 14 days, but some patients require just two to three days and others can take as long as six weeks, especially if they are being given other drugs that interact with Lydsodren, such as phenobarbital or insulin. If there is no response, dosage can be increased or mitotane can be reformulated in an oil base to increase absorption, or the drug trilostane can be used instead.
When the ACTH test and clinical signs indicate that sufficient adrenal erosion has taken place, daily use (induction phase) is stopped and lifelong “maintenance” treatment once or twice a week is begun. The ACTH test can be repeated after about a month, then one to four times a year thereafter.
If vomiting, diarrhea, appetite loss, or listlessness occur at any time during treatment, the dog may need a prednisone “antidote” pill, which should produce improvement within 30 minutes to two hours. Your veterinarian will probably prescribe prednisone and discontinue mitotane for a couple of weeks after that, before resuming at a lower dose. If there is no improvement, something else is causing the symptoms.
About half of the dogs treated with mitotane relapse at some point and require a second round of induction, and their maintenance dose may have to be increased.
Marked improvement should be seen within six to eight weeks of starting the maintenance dose, with a full reversal of clinical signs after four to six months of treatment. Usually the first improvements are more normal water consumption, urination, and appetite, and the last is hair regrowth. Muscle strength and exercise tolerance improve over the first three to four weeks.
Mitotane can be used to treat adrenal Cushing’s, but a higher dosage is needed, resulting in more adverse reactions. The average survival time in this case is 16 months.
Trilostane
Trilostane (Vetoryl®), used to treat both pituitary and adrenal Cushing’s disease, inhibits the enzyme 3-beta-hydroxysteroid dehydrogenase, which is involved in the production of several steroids, including cortisol.
Because trilostane can block aldosterone as well as cortisol, it can cause side effects such as dehydration, weakness, and electrolyte changes (low sodium and high potassium). In this case, the medication must be stopped temporarily; some dogs may also require fluid support.
For reasons that are not understood, trilostane occasionally causes acute adrenal gland necrosis, which can occur within days of starting the drug or after several months. The condition is unpredictable and is not dose-dependent. It requires prompt treatment with fluid therapy, glucocorticoids, and mineralocorticoids or it can be fatal (Addisonian crisis). This complication is permanent and irreversible, and lifelong supplementation of both mineralocorticoids and glucocorticoids will be necessary (i.e., treatment for typical Addison’s).
Trilostane is given once or twice a day with food. Side effects may be less common when given twice a day. Starting dosage is 1 to 3 mg per pound of body weight daily. Starting at the low end of that range is safest, even though the suggested starting dosage in the product brochure is higher.
Close monitoring in the beginning and after any dose adjustment is essential. Discontinue trilostane and contact your veterinarian immediately if signs of intolerance are seen. Common side effects include mild lethargy, vomiting, diarrhea, and appetite reduction, especially in the beginning. Most reactions are minor and are reversed by decreasing the dose or discontinuing therapy, but serious or fatal Addisonian reactions are also possible. Side effects should be followed by electrolyte and ACTH testing. Once symptoms resolve, the drug can be restarted at a 50 percent dose reduction.
Most dogs show decreases in drinking, urination, and appetite within one week, but some may take two months or longer. Trilostane controls clinical signs in dogs with adrenal tumors, but will not slow tumor growth.
Trilostane may be safer than mitotane, as side effects tend to be less severe and most are reversible. The risk of a permanent or life-threatening Addisonian reaction from trilostane is considered to be 2 to 3 percent.
Cost is trilostane’s main disadvantage, though monitoring costs may be less than with mitotane. Baseline cortisol levels measured 4 to 6 hours after trilostane administration may provide adequate monitoring without the need for ACTH stimulation tests.
Trilostane seems to predispose dogs to increased adrenal toxicity from mitotane, so it’s best to wait at least a month in between if switching to mitotane. When changing from another drug to trilostane, wait a couple of weeks or until clinical signs recur. This drug is not recommended for dogs with liver or kidney disease.
Ketoconazole
Ketoconazole (Nizoral®) is used to treat both adrenal and pituitary Cushing’s. This antifungal medication suppresses adrenal hormones in about 80 percent of dogs as a side effect.
A low dose is used for a week; then, if no side effects are seen, a higher maintenance dose is used. It is not possible to induce Addison’s disease with ketoconazole, so monitoring tests aren’t needed, other than after a month or so to determine if the medication is working.
Side effects can include vomiting and diarrhea, but no “antidote pill” is needed. Just discontinue until side effects go away, then restart at a lower dose.
Ketoconazole’s disadvantages are that it must be given twice a day indefinitely and its effect may be mild or temporary. This drug may reduce clinical signs in up to 30 percent of dogs with adrenal tumors, but side effects are common.
L-Deprenyl
L-Deprenyl (Anipryl® or selegiline) is used to treat pituitary Cushing’s only. It is also used to treat canine cognitive dysfunction.
L-Deprenyl works by inhibiting ACTH secretion via high dopamine levels in the intermediate pituitary area, where 30 percent of pituitary tumors are located, and may work only for dogs with such tumors. This drug has no serious side effects, but approximately 5 percent of patients experience minor nausea, restlessness, or reduced hearing. It cannot induce Addison’s disease, and no monitoring is required.
Because it’s difficult to determine whether the drug is working, and it may take considerable time to take effect, few veterinarians report good results. However, because some dogs improve and its safety margin is high, it may be worth trying in dogs with mild symptoms that are progressing slowly. L-Deprenyl can be combined with mitotane or trilostane for dogs with cognitive dysfunction, and it may increase the dog’s activity level and quality of life.
Anipryl is not recommended for dogs who also have diabetes, pancreatitis, heart failure, renal disease, or any other serious illness.
Freelance writer CJ Puotinen lives in Montana. She is the author of The Encyclopedia of Natural Pet Care and is a frequent contributor to WDJ.
Mary Straus is the owner of DogAware.com. She and her Norwich Terrier, Ella, live in the San Francisco Bay Area.
Properly used, the dog crate is a marvelous training and management tool. Improperly used, it can be a disaster. Overcrating, traumatic, or stimulating experiences while crated, improper introduction to the crate, and isolation or separation anxieties are the primary causes of crating disasters. If, for whatever reason, your dog is not a fan of the artificial den you’ve provided for him, and assuming he can’t be trusted home alone uncrated, here are some things you can do regarding his dog crate anxiety:
1. Find confinement alternatives
Every time your crate-hating dog has a bad experience in a crate, it increases his stress and anxiety and makes it harder to modify his crate aversion. Your dog may tolerate an exercise pen, a chain-link kennel set up in your garage, or even a room of his own. A recent Peaceable Paws client whose dog was injuring herself in the crate due to isolation anxiety found her dog did just fine when confined to the bedroom when she had to be left alone.
2. Utilize doggy daycare
Many dogs who have dog crate high anxiety are delighted to spend the day at the home of a friend, neighbor, or relative who is home when you are not, or at a good doggie daycare facility – assuming your dog does well in the company of other dogs. This is not a good option for dogs with true separation anxiety, as they will be no happier with someone else when they are separated from you than they are in a crate.
3. Teach him to love his crate.
Utilize a combination of counter-conditioning (changing his association with the crate from negative to positive) and operant conditioning/shaping (positively reinforcing him for gradually moving closer to, and eventually into, the crate) to convince him to go into his crate voluntarily. Then, very gradually, work your way up to closing the door with your dog inside, and eventually moving longer and longer distances away from your crated dog for longer and longer periods of time. (See “Dog Crating Difficulties,” WDJ May 2005). Note: If your dog has a separation/anxiety issue, you must address and modify that behavior before crate-training will work.
4. Identify and remove aversives.
Figure out why your dog has dog crate high anxiety. If he was crate-trained at one time and then decided he didn’t like it, what changed? Perhaps you were overcrating, and he was forced to soil his den, and that was very stressful for him.
Maybe there are environmental aversives; is it too warm or too cold in his crate? Is there a draft blowing on him? Is it set near something that might expose him to an aversive sound, like the washing machine, buzzer on a clothes dryer, or an alarm of some kind? Perhaps his crate is near the door, and he becomes overstimulated when someone knocks, or rings the doorbell, or when mail and packages are delivered. Is someone threatening him when he’s crated – another dog, perhaps? Or a child who bangs on the top, front, or sides of the crate? Maybe he’s been angrily punished by someone who throws him into the crate and yells at him – or worse. All the remedial crate training in the world won’t help if the aversive thing is still happening. You have to make the bad stuff stop.
If he’s a victim of generalized anxiety or separation anxiety and the crate aversion is part of a larger syndrome, or his stress about crating is extreme, you may want to explore the use of behavior modification drugs with your behavior knowledgeable veterinarian, or a veterinary behaviorist, to help reduce stress enough that he can learn to love his crate. Note – if your vet is not behavior knowledgeable, tell her that many veterinary behaviorists will do free phone consults with other veterinarians.
5. Take him with you.
Of course you can’t take him with you all the time, but whenever you can, it decreases the number of times you have to use another alternative. Some workplaces allow employees to bring their dogs to work with them; you don’t know until you ask. Of course you will never take him somewhere that he’d be left in a car, unattended, for an extended period of time, or at all, if the weather is even close to being dangerous. A surprising number of businesses allow well-behaved dogs to accompany their owners; if it doesn’t say “No Dogs” on the door, give it a try! Your dog will thank you.
1. Don’t punish! It may (or may not) suppress barking in the moment, but is unlikely to modify the behavior in the long run. In fact, it may actually make the barking worse or cause new behavior problems.
2. Teach your vocal dogs a positive interrupt so you can minimize their barking behavior.
3. Learn how to apply operant and counter-conditioning protocols to modify your dogs’ barking when you can’t or don’t wish to manage the behavior.
4. Have reasonable expectations: accept barking is normal and appropriate for dogs. Identify times when you can allow your dogs to vocalize.
It’s feeding time at the Miller household. All is calm until I pick up Scooter’s bowl to carry it to the laundry room where the little Pomeranian can eat without harassment from the larger dogs. As I lift the bowl from the counter, Scooter erupts with high-pitched barking and spinning, and Lucy the Corgi joins in with her deeper-but-still-sufficiently irritating vocals. It’s more of an annoying bit of ritual than a dangerous or disturbing one, but it’s annoying just the same, and one that would be nice to extinguish.
But how does one modify behavior if the protocol requires the offering and removal of reinforcement based on the subject’s behavior, when there are two subjects, and reinforcement for one automatically reinforces the other? Stated in plain English, how do I get two (or more) dogs to stop barking when rewarding the quiet one also rewards the barking one?
When One Dog Starts Barking, the Rest Follow
If I set the bowl back down on the counter when both dogs bark, I’m using negative punishment; the dogs’ behavior of barking makes the good thing – delivery of their meal – go away. When the dogs stop barking I use positive reinforcement; the dog’s quiet behavior results in a good thing: I pick up the bowl and proceed with delivery of dinner.
Now, here’s the dilemma: When I pick up the bowl, Lucy stays quiet, so I should positively reinforce that by continuing with dinner delivery. But Scooter starts barking again; I need to abort delivery so I’m not reinforcing Scooter’s barking. But if I set the bowl back down, I’m punishing Lucy for being quiet. Get it?
The answer to the dilemma is this: I can modify the behavior of only one dog at a time. I need to select which dog I want to work with first, and figure out how to manage the other dog’s behavior until I’m ready to work with her. In this scenario, I might change my dog-feeding routine by putting Lucy in my office before I begin food preparation so I can work with Scooter’s barking behavior. After he gets his dinner, I can let Lucy out to join the rest of the group, and feed all of them.
When Scooter no longer barks at food delivery time, I can try reintroducing Lucy to the mix. If her barking re-triggers Scooter’s barking, then I might need to put Scooter away while I work on modifying Lucy’s barking. When each can handle dinner delivery without barking, then I can try them together.
Counter-Conditioning Multiple Dogs at Once
Many multi-dog training programs break down because owners, understandably, aren’t always willing to work with the dogs separately. The prospect of implementing multiple behavior modification programs for multiple dogs can be quite daunting. We’re lucky only two of our five dogs bark at dinnertime. If all five joined in, the cacophony of barking would be overwhelming, not to mention the prospect of working with each of five dogs to modify barking behavior. They might never get fed!
Yet, individual modification work is almost always necessary for success with behaviors that involve multiple dogs. One dog’s barking just sets the other(s) off if the other’s barking hasn’t been solidly modified. Perhaps the two most common examples of multi-dog barking are when an owner walks two or more dogs on leash at one time, or when multiple dogs in a home (or in the yard) are aroused by some stimulus, such as someone at the door, someone walking past on the sidewalk, a squirrel or cat running across the yard or up a tree, a car going by . . .
I see the pained expression on my clients’ faces when I suggest to them that they need to walk their dogs individually, or at least with separate handlers. In many households, one person is in the habit of taking both (or all) dogs for a walk at the same time. I can see them doing the math in their heads; a 30-minute walk per day with three dogs has suddenly compounded into three 30-minute walks, or 90 minutes per day. That equals 10.5 hours per week instead of 3.5 hours. Wow. Who has that much extra time to devote to dog walking?
Still, it’s important. When dogs-on-leash are barking at an outside stimulus, such as another dog or a passing car, my favorite approach to modification is counter-conditioning. The instant your dog sees another dog (or the approaching vehicle), feed bits of chicken (or other very high-value treat), preferably before your dog begins barking. Pause, let him look at the approaching dog (car), and quickly feed more chicken, again before he barks. Continue with your pause/look/treat procedure until the dog (or car) has passed. Then resume your walk until the next dog (car) comes along.
Over time, your dog will learn that the appearance of another dog/car makes you feed him chicken, and instead of barking, he’ll look to you for chicken. This works whether the stimulus causing him to bark is a dog, a car, a kid on a bicycle, or anything else. In time, as his “stimulus/chicken” association becomes very strong, you’ll be able to gradually – and significantly – reduce the amount of chicken you have to feed. In time, you’ll be able to leave the chicken home and just use his regular everyday treats to reinforce his looks at you when a target passes.
As simple as this process is, it’s virtually impossible to do it with two dogs at the same time. The timing of your treat delivery is critical; it must happen the instant after your dog sees the stimulus but before your dog starts to bark. You simply can’t manage two potential barkers and get the timing right for both. Hence the mandate to walk one dog at a time – or at least one dog per handler – if you’re serious about getting the barking under control. When you have solidly established the conditioned emotional response (CER) – the “where’s my chicken look” – for each dog separately, you can begin to walk them together.
Multi-Dog Training: Positive Interrupt
You can modify multi-dog “someone’s at the door” barking in a similar fashion – but it’s harder because all the dogs are usually in the home. You could do a lot of one-at-a-time set-ups with the other dogs out of earshot. (See “Knock, Knock,” WDJ February 2010). Still, chances are when someone comes a-knockin’, at least one of your multiple dogs may bark, which just might set everyone off. The same is true with outside/backyard stimuli. Despite your best efforts to counter-condition, the arousal behavior of multiple dogs is likely to cause mutual escalation or arousal, and barking will happen.
For those times, a positive interrupt is a powerful tool. I use a voice cue (“Over here!”) as a positive interrupt for an individual dog, but in the chaos of multi-dog barking, a louder signal is called for. If you are blessed, as I am, with the ability to give a shrill mouth-whistle, that can work. If not, there are wonderful whistles for sale that are so loud you’ll need to cover your ears when you blow them, or risk damage to your hearing. My favorite is the Storm Whistle. You might want to buy several, so you can stash them in strategic locations around your house and yard.
You’ll want to “charge” your whistle in the same way you charge a clicker, to give your dog a very positive association between the sound of the whistle and something wonderful. I tend to fall back on chicken as my favorite “something wonderful” – dogs usually love it, and it’s relatively low-fat, low-calorie, so you can use it generously without adding too many pounds to your dog, and with a low risk of tummy upsets.
Charge the whistle one dog at a time. With one dog close to you and the others put away out of earshot, blow the whistle (not too loudly) and feed a treat. Blow the whistle, feed a treat. Repeat many times. When your dog makes the connection between whistle and chicken, you’ll see his eyes light up at the sound, and he’ll be looking for the treat. Next, go out in the yard where he can be farther away from you, and repeat your whistle/treat routine, until the sound of the whistle brings him running for a treat even when he’s some distance away, sniffing the ground. Now put him away and try it with the next dog. When all dogs are “charged,” try it with two dogs at a time, gradually adding dogs to the group until your entire pack will interrupt what they’re doing and come running to you at the sound of the whistle. (By the way, this doubles as a great recall tool as well!)
Now you’re ready to try it for real. If you’re confident your dogs will respond, give it a try with the whole pack. If you think that’s too much for your canine pals, start your real life trials one, or maybe two dogs at a time, just like you did with charging the whistle. Arrange a set-up that you know will trigger your dog(s) to bark. Have your whistle handy. When the barking starts, blow the whistle, and reward your dogs generously when they stop barking and come running to you. Then pat yourself on the back.
Continue practicing with set-ups for as many different stimuli as you can think of. The more you practice, the better your dogs will respond when real-life stimuli trigger a bout of barking. If you’re really good, your dogs may start running to you in anticipation of the whistle/treat game when they see or hear stimuli that used to cause barking. When that happens, you deserve to reinforce yourself with dinner and a movie.
Pat Miller, CBCC-KA, CPDT-KA, CDBC, is WDJ’s Training Editor. Author of numerous books on positive dog training, she lives in Fairplay, Maryland, site of her Peaceable Paws training center, where she offers dog training classes and courses for trainers.
Thanks to Sarah Richardson, CPDT-KA, CDBC, Chico, California, for modeling for this article.
In February 2010 my Border Collie, Daisy, became one of an estimated six million dogs diagnosed with cancer each year.
Chemotherapy. My stomach tumbled to my feet. The diagnosis was scary enough; how could I possibly consider chemotherapy? I had visions of a treatment worse than the disease itself.
As it turns out, my preconceptions of chemotherapy were far worse than its reality. Chemo hasn’t cured my dog – more on that later – but it’s given us more than 18 months (and counting) of joyful, quality time together. It’s even given Daisy a dozen new friends and routines to look forward to, in the form of her oncologist and chemotherapy technicians and the special things they do to make her comfortable on her “chemo days.”
Chemotherapy for Dogs: Basics
Chemotherapy at its most basic definition is simply chemical treatment of an ailment. In this sense, we use chemotherapy everyday: antibiotics, NSAIDs, vitamins, herbs. Chemotherapy for the specific treatment of cancer involves infusing the dog’s system or a specific place in the dog’s body with cytotoxic chemicals in an attempt to destroy the cancer cells while hopefully doing as little damage as possible to normal healthy cells. Other than a few specially designed drugs for a couple of specific cancers, chemotherapy drugs attack cells in the process of rapid growth or division.
Cancer chemotherapy was developed in the 1940s when researchers became aware of the effects of mustard gas, which was being used as a chemical warfare agent. Those exposed to the gas were found to have very low white blood cell counts and researchers reasoned that if the chemical had an effect on the rapidly growing white blood cells, it might have a similar effect on the fast growing cells in some of the blood cancers. This led to further research and development of similar drug protocols.
Daisy has transitional cell carcinoma (cancer of the bladder). It is not curable, but it is treatable. I had to ask myself why I would treat her with toxic drugs. For this type of cancer, the first reason is to prevent metastasis – the spread of cancer to other parts of the body. The second reason was to control the disease and thereby increase her longevity and enhance her quality of life. For other types of cancer, chemotherapy might be used to reduce the size of the tumor so that surgery can be performed. Chemotherapy can also enhance the effectiveness of other cancer destroying treatments such as radiation. In some cases, it can rid the body of the disease, though this goal is not realistic at this time for many with the disease.
The goal of chemotherapy drugs is to kill the cancerous cells, while administering a dose that causes “tolerable” harm to the body’s normal tissues. Since a distinct trait of cancer cells is that they grow at a faster rate than most normal cells, chemotherapy agents usually affect the process of replication of these rapidly dividing cells by interfering with DNA or RNA at the cellular level. Most agents kill cancer cells by affecting DNA synthesis or function, a process that occurs during the cell cycle. The agent binds to the DNA and alters the replication process; the cellular activity is thereby halted and the cell dies. There is a balancing act between destroying as many malignant cells as possible and leaving enough normal cells to recover.
There are more than one hundred chemotherapy drugs being used to treat canine cancers and more are being developed all the time. Many years of research have resulted in established (but evolving) treatment protocols – treatment plans developed for a specific cancer type in which drugs are selected for their unique and complementary cancer-fighting properties and administered in a particular order and schedule. Combination chemotherapy is a protocol in which different drugs are rotated or given concurrently. With this approach, the drugs are given so as to attack the cancer cells in different ways thereby decreasing the possibility that the cancer cells will survive and become resistant to the beneficial effects of the agents.
There are many factors that your dog’s oncologist will take into account when selecting the protocol to use for your dog, including the type and extent of the cancer, the nature of the agents, published evidence of their efficacy, any potential adverse reactions, and your dog’s medical history and overall well-being. Your dog’s breed, too, may affect the protocol; some breeds with the MDR1 mutation cannot tolerate certain chemotherapy agents. (Get a list of commonly affected breeds and a test to identify affected individuals here.) And of course, the oncologist’s own training and experience plays a part in the decision.
If an oncologist does not see a response within a certain timeframe, the particular agent may be determined to be ineffective and another protocol may be administered or the treatment halted. The oncologist may even develop a protocol that isn’t standard but is the best way to treat your dog.
The common routes of drug administration are by mouth (orally), or by injection, which can be given through a vein (intravenous), into a muscle (intramuscular), or under the skin (subcutaneous). These are systemic treatments that travel throughout the body to reach the cancer cells wherever they may exist. More recently, other methods have been developed to increase the local concentration of the agent at the tumor site. Such site-specific applications can direct the agents to the affected areas of the abdomen, lungs, bladder, the central nervous system, and the skin. This process can reduce the systemic effects as well as provide a stronger action of the drug at the disease location.
Your dog’s specific dosage of a drug will be generally based on his body weight; other factors include your dog’s overall health and sensitivity to drugs. The dose must be high enough to be medically effective but not so high as to cause unnecessary damage to healthy cells.
Most plans begin intensive therapy with higher and more frequent doses of the agent in attempt to beat the disease back. The duration of the protocol depends on the type of cancer, the extent of disease, and how responsive it is to the treatment; the general recommendation is to administer 2-3 doses of a particular agent before determining if it is having an effect. Treatment periods can range from weeks to years. While the sound of “years of chemotherapy treatment” may sound daunting, remember that it means the treatment is working.
In addition to the chemotherapy administration itself, other exams and tests will be performed during the course of treatment. Some tests are done to see if your dog can safely receive treatment; others, such as ultrasounds, urinalysis, x-rays, CT scans, MRIs, and scopes monitor overall health and cancer status.
A routine checkup will take place during every visit. Like a report card, the following information should be relayed: your dog’s overall well-being, medications given, any changes in eating/drinking/elimination habits, any sign of illness, change in behavior, change in tumor (if visible). Report any changes to your veterinarian’s staff, no matter how insignificant the changes may seem. Thorough awareness and inspection of your dog is your responsibility. Veterinary technicians will perform a physical examination that will include obtaining heart rate, weight, and a blood sample.
Because many agents also affect healthy cells and organs, your dog’s laboratory data will be checked before each chemotherapy administration. In addition, an assessment of the effects on organs may be performed on a periodic basis. Abnormalities in any of these values may require dose adjustments or delay of therapy.
Clinical Trials of Cancer Drugs
The identification and development of effective nevv anticancer drugs is an ongoing process. Agents with a potential for antitumor activity are evaluated in clinical trials. Many veterinary teaching hospitals run such trials. lfyou are interested in having your dog participate in a trial, ask your oncologist or check caninecancer.com for a list of links.
Weighing the Chemotherapy Option
– Is the expectation of the treatment worse than the treatment itself?
– How healthy is my dog?
– How does my dog handle trips to the veterinarian?
– How sensitive is my dog’s gastrointestinal system?
– Do l have emotional, financial, and/or time commitment constraints that will lessen my ability to commit myself fully to my dog?
Possible Chemo Side Effects on Dogs
Every dog will be different in his or her ability to handle treatment. Some dogs will experience side effects; some won’t. Side effects tend to be temporary, spanning just the amount of time that it takes normal cells to be replaced or to repair the damage incurred from the chemo.
Canine oncologists have considerable experience with many of the standard drugs and how they affect dogs; they may prescribe medications to help prevent known potential issues. As with the administration of any drug, there can be a severe immediate reaction; this is extremely rare. This is why your dog will be monitored closely during the administration of the drug and observed for about an hour afterward. Other side effects can appear 1 to 3 days after administration and include lethargy, decreased stamina, diarrhea, nausea, and or/vomiting.
To counter the potential for nausea and vomiting, anti-nausea medication such as metoclopramide is often administered along with the chemotherapy agent or drugs such as Cerenia will be dispensed to give at home should these symptoms occur. Pepcid AC may also be suggested to prevent stomach upset. Bland diets can also help.
Guardians need to learn what the potential side effects are for the drugs their dog is receiving and how to watch for them. At times, it can be difficult to determine if a side effect is caused by the treatment or from the disease itself. Symptoms are especially difficult to evaluate during the beginning stage of treatment when there is nothing to compare them to. A day or two of nausea or a vomiting episode or two is not unexpected and is rarely dangerous. Notify your veterinarian immediately if your dog does not eat or drink for one day or longer, or if vomiting is continuous and water cannot be kept down, or if you notice blood in vomit or diarrhea. Record and report all your observations to the oncologist. If your dog does have a reaction, you may wonder whether to continue treatment; remember that the dosage can be adjusted or a different drug selected for use.
Unfortunately, the treatment drugs cannot distinguish between cancer cells and non-cancer cells. As a result, the destruction of the fast growing cells of the bone marrow and gastrointestinal tract becomes a concern. In addition, some drugs may damage the reproductive tract (not a problem in neutered or spayed dogs); others may affect specific organs such as the heart, liver, and/or kidneys and thus require frequent monitoring.
Some chemotherapy drugs affect the bone marrow, thus affecting the body’s ability to produce new white blood cells (WBCs). Your dog’s WBC count will generally be at its lowest 5 to 7 days after treatment. The lowering of the white blood cell count can make your dog more susceptible to infections, which generally arise from bacteria that normally live in the dog’s intestinal tract and on the skin, not from the environment. (So let your dog do the things he or she usually does, just use common sense and avoid known hazards such as dog parks with an outbreak of a contagion). Your veterinarian may also prescribe prophylactic antibiotics to prevent the possibility of infection if your dog’s neutrophil (a component of white blood cells) count is low (neutropenia), even if there is no evidence of infection.
Early detection of infection is important so that antibiotic treatment can be started immediately. Signs of infection can include loss of appetite, vomiting, diarrhea, lethargy, or depression. To help monitor for infection, familiarize yourself with how to take your pet’s temperature. Contact your vet immediately if the temperature is higher than 102.5°F (or otherwise indicated by your veterinarian), as a fever is an indication of infection. A dog’s normal temperature is about 100.5°F to 102.5°F. Again, severe vomiting or diarrhea, bloody diarrhea, or lethargy are indications you should contact your veterinarian immediately; severe infections may require hospitalization for intensive supportive care.
The cumulative effects of multiple doses of certain chemotherapy drugs can cause permanent side effects; if the risks outweigh benefits, treatment should be discontinued. Certain powerful drugs can only be used a limited number of times before the risk of toxicity to certain organs becomes too great. Other drugs may be inappropriate because of reactions or debilitating side effects. Sometimes, the cancer develops a resistance to the drug. The list of effective chemotherapy agents may diminish as treatment progresses; this is where the knowledge, experience, and creativity of your dog’s oncologist come in.
Does Fur Fall Out During Chemo?
The first question many people ask about canine chemotherapy is whether the dogs lose their hair! Most breeds have fur, not hair, and it grows and sheds in a cycle, not continuously. However, some curly-coated breeds with hair (such as Poodles) may experience hair loss. Chemotherapy drugs target fast growing cells (like hair); fur is not a fast growing cell. Sometimes dogs will lose their whiskers and shaved areas may not regrow as quickly, but that’s about it.
Find out how else chemo for dogs is like chemo for humans here.
Living with a Dog Undergoing Chemotherapy
As with humans being treated with chemotherapy, people and pets are not thought to be at risk from living and interacting with a chemotherapy-treated dog. Most chemotherapy drugs clear the system through the urinary and/or intestinal tract within 48 to 72 hours of administration. To limit exposure of these drugs to yourself and other pets, try to have your dog eliminate in one particular area, away from areas where children play and other pets frequent. Wear disposable gloves to pick up feces immediately and place in a plastic bag and seal before disposal. If possible, thoroughly rinse areas of elimination with running water to dilute any chemical residue.
If your dog vomits or eliminates in the house, wear disposable gloves and use paper towels to clean up as much of the waste as possible. Again, bag the gloves and soiled paper towels before disposing. Depending on the location of the accident, you may want to use a thorough water rinse to clean the area. If your pet is receiving daily doses of a drug that you administer orally, the drugs should be handled only while wearing protective gloves (and kept out of the reach of children and other pets). Always wash your hands after handling medications or waste! If any member of the household is pregnant, trying to become pregnant, or immune-compromised, she should not handle any treated animal’s waste or anti-cancer medications.
Paying for a Dog’s Cancer Treatment
Chemotherapy treatment can be expensive as it involves professional time and expertise, the high costs of the drugs themselves, the duration of treatment, the associated procedures and diagnostics, as well as the removal of biomedical hazardous waste (including the leftover drugs, the catheters and needles used to deliver the drugs, the technicians’ smocks and gloves, etc.). Most veterinary centers will bill per treatment, not in one lump sum. If you have pet insurance, check your policy; some plans cover treatment. CareCredit also offers special financing for approved veterinary procedures. On her blog, Dr. Nancy Kay has a great resource page for “Financial Assistance for Veterinary Care.” This information also appear in her book, Speaking For Spot. Ask for an estimate of expected costs so that you can evaluate the financial impact and discuss any financial concerns you have with your veterinarian so that he or she can offer the best treatment options based on your budget.
Questions About Chemo to Ask Your Vet
1. What is the life expectancy without treatment?
2. What is the gained life expectancy with treatment?
3. What chemotherapy agents will my dog be given?
4. How are they administered?
5. What is the process?
6. How is the effectiveness evaluated?
7. How frequently will treatment be given?
8. How long will my dog receive treatment?
9. What is the estimated cost of treatment?
10. What side effects might my dog experience?
11. What clinical signs should I be concerned about?
12. What signs require me to bring my dog in immediately for examination?
13. Who should I contact after office hours if my dog has symptoms that worry me?
Supporting Chemo Recovery
Your dog’s body must work harder to maintain good health; not only is it battling a disease, it is working to repair the collateral damage from the chemotherapy agents.
Be especially aware of symptoms of pain; as we know, dogs are especially good at hiding any signs that they might be hurting. But pain can cause stress and stress can be detrimental to your dog’s overall health and healing process. Work with your veterinary team to prevent and treat it.
The presence of cancer can result in significant alterations in your dog’s digestion. There are some general concepts that can be followed to provide good nutritional support: provide a variety of foods that are aromatic and tasty; minimize the feeding of simple carbohydrates (starches and sugars – studies have shown these to be fuel for cancer); give foods with high quality protein sources; and consider the addition of omega 3 fatty acids. While optimal nutrition is ideal, it may come down to feeding whatever your dog will eat. There are a myriad of supplements that claim to be of benefit, but many of these are unfounded and unproven; discuss any supplements that you consider giving your dog with the oncologist.
If your dog is on chemotherapy for any period of time, you may find she needs non-cancer treatment or medications. While on chemotherapy, no regular vaccinations should be given, though heartworm and flea preventatives can be given as long as not contraindicated with the chemotherapy or your dog’s overall health. Always coordinate regular veterinary care with your oncologist.
Other areas of support you might want to consider include acupuncture, chiropractic, herbal, and homeopathic remedies. Daisy receives acupuncture twice a month and takes herbal supplements as prescribed by her holistic veterinarian, who works closely with her oncologist to check for drug interactions. Her herbal supplements are ceased 24 hours before and after chemotherapy administration to reduce the potential for any interactions.
One of the most important aspects of treatment is to maintain a positive attitude and keeping your dog’s life – and your life – as normal as possible. Exercise within your dog’s abilities, play, and enjoy every moment. While we have to remember the clinical reality, it’s best to focus on your dog’s reality!
Be Your Dog’s Advocate
– Be an informed guardian.
– Research your dog’s specific disease.
– Discuss your findings with your dog’s oncologist.
– Join or start an online support group.
– Record every detail about your dog’s behavior during treatment.
– Act quickly if immediate medical attention is needed.
– Familiarize yourself in advance about the potential side effects.
Living for Today, Preparing for Tomorrow
Chances are there has been research and studies (try searching online using Google Scholar) on your dog’s particular kind of cancer. These studies will often include statistics such as median survival times and side effects of particular agents. They can be disheartening or encouraging. Do discuss your findings with your dog’s oncologist, but remember there is no crystal ball to predict how your dog might react or respond. Each dog is unique and each cancer that develops is unique. A disease that develops in one dog may not be treatable in another for a variety of reasons such as location of disease, the dog’s age and health, and the cost and availability of treatment. That said, it can be helpful to review the statistics, however extensive or limited, and use them as guidelines for weighing potential risks and benefits.
Realistically, there are few cancers that can be cured by chemotherapy. Some can go into remission (no detectable evidence of the disease), and even multiple remissions (such as with lymphoma). Others can become static (reduction and or no advancement of the disease).
Remember, if you decide to embark on the chemotherapy route, you can stop at any time. When I started treatment with Daisy, my guiding principle was that if it affected her quality of life in any way, we would cease therapy immediately. She’s been receiving chemotherapy for over 16 months now, including intravenous mitoxantrone, carboplatin, and vinblastine; we also tried the oral drugs Leukeran (chlorambucil) and Palladia. Unfortunately none of these had the desired effect of combating the disease, but fortunately they did not have any detrimental affect to her well being. She’s also received piroxicam (an NSAID that has anticancer properties) for over a year; we’re not sure if this had any effect on the disease, but it did seem to have a palliative effect (she now takes Deramaxx instead).
There was a period when I did stop treating her with conventional chemotherapy agents, but that was because we had run out of drug options for her particular type of cancer. At that point, I put her on an herbal chemotherapy as recommended by her holistic veterinarian. She continues taking it now in conjunction with a special combination protocol of two chemotherapy agents as developed by her oncologist. We’re now at 18 months since diagnosis (her prognosis was less than a year) and I can joyfully report that her disease is static and she is happy and feisty. She comes home from her oncology visits ready to play frisbee.
The author wishes to extend her heartfelt thanks to Daisy’s amazing and caring oncologists, Jeffrey N. Bryan, DVM, MS, PhD, DACVIM (Oncology), at the College of Veterinary Medicine, University of Missouri and Martin Crawford-Jakubiak, MLAS, DVM, DACVIM (Internal Medicine, Oncology), and his wonderful team at Sage Centers for Veterinary Specialty and Emergency Care in Concord, CA.
Author Barbara Dobbins is a dog trainer on hiatus who has been inspired to return to school to study veterinary oncology.
Resource guarding in dogs is a natural, normal behavior. In fact it’s a natural behavior for most warm-blooded animals. Even we humans guard our resources—sometimes quite fiercely. Think about it. We lock our doors. Store clerks have loaded rifles under checkout counters, while homeowners keep shotguns and baseball bats leaning in the corner by the back door. Companies hire security guards. Banks keep valuables in vaults. Some of us get insanely jealous if someone pays too much attention to our significant other. I could go on…
Dogs guard their resources as well, sometimes quite fiercely. This is most troublesome when they guard those resources from humans, but resource guarding can also get them in hot water when they guard from other dogs. That said, some dog-dog resource guarding behavior is quite appropriate and acceptable. The wise dog owner not only knows the difference between appropriate and inappropriate guarding, she also knows when and how to intervene, manage, and modify.
Examples of Resource Guarding in Dogs
If dogs didn’t guard their resources from other dogs they’d be in danger of starving—both in the wild and in multi-dog households. It’s this survival instinct that triggers everything from the canine dirty look known as a “hard stare” to the ferocious blood-letting, sometimes fatal battles that can occur when dogs fight over valuable, mutually-coveted resources: food, toys, objects, locations, beds, and human attention.
There are several different scenarios that can occur when one dog chooses to guard something from another dog, ranging from a very healthy, normal interaction, to those that risk the very lives of one or more of the combatants:
1) Ideal: Dog A and Dog B are both appropriate
The ideal resource-guarding scenario probably plays itself out frequently in multi-dog households, dog parks, doggie daycares, and anyplace dogs randomly gather. It looks something like this: Dog A is chewing happily on a (insert any valuable resource here). Curious, Dog B approaches. Dog A gives Dog B “the look.” Dog B quickly defers, saying, “Oh, excuse me!” by calmly turning and walking away. No harm done. Much of the time the dogs’ owner isn’t even aware that this occurred.
2) Second Best: Dog B is inappropriate but Dog A defers
Dog A is chewing on (insert resource). Dog B approaches. Dog A gives Dog B “the look.” Dog B gives Dog A “the look” back. Dog A defers, “Oops, sorry!” by dropping the resource and leaving. Dog B was inappropriate, but Dog A didn’t want to argue about it. The danger here is that somewhere along the line Dog A may get fed up with Dog B’s inappropriate behavior and decide not to defer.
3) Now We’re in Trouble, Part I: Dog A is inappropriate
Dog A is chewing on (insert valuable resource). Dog B approaches. Dog B would defer if warned, but rather than giving “the look,” Dog A leaps into action and attacks without giving Dog B the opportunity to defer.
4) Now We’re in Trouble, Part II: Dog B is socially inept
Dog A is chewing on (insert valuable resource). Dog B approaches. Dog A gives “the look.” Dog B is oblivious, and keeps blundering forward, until Dog A feels compelled to escalate the intensity of his message, to aggression if necessary, to get his point across.
5) Now We’re in Trouble, Part III: Dog B is inappropriate and Dog A doesn’t defer
Dog A is chewing on (insert valuable resource). Dog B approaches. Dog A gives “the look.” Dog B gives Dog A “the look” back. Instead of deferring, Dog A takes offense and escalates his aggressive behavior to maintain possession of his resource. Dog B reciprocates with increased aggression, and a serious fight ensues.
The same five scenarios can apply to other resource guarding situations—the dog who doesn’t want to share his sticks or toys; who becomes tense if another dog approaches him on his bed; or who claims his owner’s total and undivided attention. So whether it’s food or some other valuable possession your dog is guarding, what do you do about it?
Be Aware of Resource Guarding Tension Between Dogs
First, you have to be aware of the resource guarding tension. It’s hard to miss in Scenarios 3, 4, and 5, but if you have dogs engaged in one of the first two you may have overlooked it. Time to sit up and take notice! With Scenario 1, where both dogs respond appropriately, all you need to do is keep an eye on things and breathe a sigh of relief. As long as the pattern repeats itself, you needn’t worry. You just need to stay calmly observant and take note if the pattern changes—if, for example, Dog B is slower to defer over time, which may cause an increase in Dog A’s tension and possibly escalate to higher-intensity resource guarding. Many dogs live happily together their entire lives politely signaling and deferring in relation to valuable resources. That’s how it’s supposed to work—perfectly appropriate and normal.
If you see subtle signs of increasing tension, however, or if you see Scenario 2 behavior, where Dog B is bullying Dog A into giving up the resource, you have potential trouble brewing. It’s possible that Dog B will calmly defer for the rest of the dogs’ lives together. You could continue to observe, and intervene only if things start to escalate. Maybe it never will. Or you could intervene with management and/or modification now, before you have significant relationship damage to repair, and a more difficult behavior modification challenge.
Of course, anything more dramatic than Scenario 2 behavior requires immediate action in the form of management and, if you choose to do so, modification.
You Can Manage Resource Guarding in Dogs
I’m a huge fan of management. If your dogs’ list of guardable items is relatively short and the dog-dog guarding interactions are reasonably predictable, then management may be a realistic option. Feed meals to your dogs or give them pig ears only when they are safely crated or closed in separate rooms. If you have a toy guarder, do toy-play with the dogs separately, and put coveted toys away when the dogs are together. Case closed.
Modification is in order, however, if battles grow increasing likely to erupt unexpectedly over an ever-growing list of miniscule triggers, such as a crumb dropped on the floor, a preferred resting spot on the rug, the hallway to the kitchen, equitably delivered treats to both dogs, or a rapidly growing radius around a valued human. Of course you’ll manage in the meantime, but since management always carriers a risk of failure and guarding battles can be fierce, the more generalized the guarding, the more critically important it becomes to convince your dogs to act appropriately with other dogs in the presence of high-value resources.
Modify Your Dogs’ Behavior to Deal With Resource Guarding
Aggression is caused by cumulative stress that pushes a dog over his aggression threshold. We’re all grumpier when we’re stressed. (See “Understanding Aggression in Dogs,” WDJ October 2010). Begin your modification program by minimizing as many other stressors as possible in your dogs’ world. That includes creating structure and predictability in their lives; exploring and treating any possible medical conditions that may cause pain or distress; and eliminating the use of any coercive or pain-causing training tools and methods (shock, choke and prong collars, physical or harsh verbal punishment).
At the same time, incorporate calmness-inducing products and procedures such as increased aerobic exercise, the “Through a Dog’s Ear” recordings, Thundershirts or Anxiety Wraps, calming massage, and TTouch.
There are a few different options for modifying resource-guarding behavior between dogs. You can classically condition Dog A (the guarder) to love having another dog around him even in the presence of valuable resources; you can operantly condition Dog A to perform a different response when he’s in possession of a valuable resource and another dog approaches; and you can operantly condition Dog B to avoid the guarder when he has a valuable resource. Here’s how each of these work.
Counter-Condition for Resource Guarding with Dog A
The point of counter-conditioning is to change Dog A’s emotional response to the proximity of Dog B in the presence of a guardable resource. This procedure will require dogs with very solid sit-stays and down-stays. Alternatively, you can use tethers. It’s critically important that Dog A not be triggered to guard during these training sessions; awareness of threshold distance and the dogs’ proximity to each other is paramount.
Step 1: Start with the two dogs sitting a few feet from each other—farther, if necessary to avoid guarding behavior. Have a bowl of pea-sized, high-value treats. Give a treat to Dog B (the non-guarder), and then give one to Dog A, accompanied by happy-voice praise. If the dogs are so far apart you have to walk some distance to get to Dog A, start praising as you walk. Repeat until you see Dog A brighten noticeably when Dog B gets his treat; this tells you he’s made the association between Dog B getting a treat and the next delicious treat coming to him. This is a “conditioned emotional response” (CER)—the physical manifestation of the emotional change that happens because of the pairing between the presence of the other dog and the arrival of a high-value treat.
If you start with the dogs far apart, when you have established a consistent CER with Dog A, gradually move them closer together, continuing with the counter-conditioning and achieving CERs at each new distance until the dogs are happily taking treats a few feet apart. Depending on your dogs, this could take one session or many.
Step 2: Have a bowl of high-value treats. Hang out with Dog A in a good-sized quiet room with the door closed—watch TV, read a book, work on the computer—but don’t feed him any treats. In fact, ignore him completely. After 20 to 30 minutes, bring Dog B into the room on leash and have him sit. Feed him a treat, then spend 20-30 seconds giving generous treats and praise to Dog A. Then remove Dog B from the room.
At varying intervals, bring Dog B back into the room and repeat the procedure—always bringing Dog B into the room before you make any move to reach for the treats in the bowl. Repeat until Dog A looks consistently happy—the CER—as you move to bring in Dog B.
Step 3: Repeat Step 2, but this time Dog A is in possession of a guardable resource—a bone, a toy, a favorite bed. If there are things he guards less intensely than others, start with a lower-value resource.
Tether Dog A with his resource as far from the door as possible, and hang out for another 20 to 30 minutes before bringing in Dog B. Step in the door with Dog B, have him sit, feed him a treat, and then do your 20- to 30-second praise-and-treat routine with Dog A. Repeat until you have a consistent CER—Dog A brightens happily when you enter the room with Dog B.
As you do these repetitions, occasionally encourage brief eye contact between the dogs several times at each distance, so that trigger gets built into the procedure. If eye contact triggers significantly greater intensity from Dog A, stay at the door until that intensity goes away and you are getting consistent CERs even with eye contact.
Gradually move closer with Dog B, obtaining consistent CERs from Dog A at each new distance before moving closer again. Remember to look for and reward some eye contact between the dogs.
When you have closed the distance by half, mark that spot and start over again at the full distance, but this time with Dog A untethered. This should not trigger any tension from Dog A, and you should be able to move closer to him with Dog B more quickly than before.
Step 4: Repeat Step 3 with the same value resource, in all the rooms in the house, until Dog A displays consistent CERs everywhere.
If you have multiple dogs who Dog A guards from, repeat Steps 1 to 4 with each of the dogs. Then do the same thing with multiple dogs in the presence of Dog A and a low-value guardable resource.
Step 5: Go back to Step 3, again with Dog A tethered, but now in possession of a somewhat more valuable resource. Repeat all steps with all dogs, individually at first, then in larger groups, until Dog A offers consistent CERs regardless of what dog or what room. Continue up the resource-value ladder until Dog A shows no sign of tension
Step 6: Do occasional “cold trials” without the set-up and repetition—a deliberate “management failure” in which counter-conditioning meets real life. Do at least one cold trial per day, and if you see tension reappearing, go back and do repetitions of the procedure at whatever step is necessary for your dog to regain his equilibrium. Then move through the steps to completion—probably much more quickly than the first time through.
Operantly Condition Dog A to Address Resource Guarding
Resource-guarding in dogs lends itself beautifully to the “Constructional Aggression Treatment” (CAT) operant conditioning protocol developed by Dr. Jesus Rosales Ruiz and Kellie Snider, MA, a few years ago at the University of North Texas. (See “Build Better Behavior,” WDJ May 2008). Our Dog A gets tense and eventually aggressive because he is concerned that the approaching dog is a threat to his valuable resource. These aggressive distance-increasing signals are often successful in making the other dog go away, hence they are reinforced, and behaviors that are reinforced are repeated.
To use the CAT procedure, tether Dog A with a low-to-moderate-value guardable resource, and approach from a distance with Dog B. If you know that Dog A begins showing signs of guarding at a distance of 15 feet, start at 25 feet. As you approach, watch Dog A for any small sign of tension. The instant you see it, stop with Dog B, mark the spot, and wait. As soon as you see any decrease in Dog A’s tension, any sign of relaxation, quickly turn and walk away with Dog B, back to the 25-foot distance.
Pause there for at least 15 seconds (longer, if you think Dog A needs more recovery time), and then repeat, returning to the marker at the spot where you stopped before. Continue these repetitions until you see no sign of tension from Dog A when you arrive at the marker with Dog B.
On your next approach move four to six inches closer and mark that spot. You will likely see Dog A display signs of tension again at this distance. Repeat approaches and departures at this distance until the tension is gone, then decrease distance slightly again.
What you are doing with this procedure is teaching Dog A that a new behavior—acting calm and relaxed—makes the threat to his resource go away. As he continues to deliberately act calm and relaxed, he actually becomes calm and relaxed, and eventually no longer feels threatened by the approach of Dog B. Ideally you will see “crossover” behavior, where he acts very friendly and affiliative as Dog B approaches, offering distance-decreasing signals instead of his previous repertoire of distance-increasing signals. When you’ve worked through the procedure with low-to-moderate-value resources, repeat with high-value resources.
With counter-conditioning, you change your dog’s emotional response, and as a result his behavior changes. With operant conditioning (CAT), you change your dog’s behavioral response, and as a result his emotional response changes.
Operantly Condition Dog B to Counteract Resource Guarding
You can also operantly teach Dog B a new behavior in the presence of Dog A and a valuable resource. This is a useful second line of defense, in combination with modifying the behavior of the guarder. You can teach Dog B to withdraw on your cue; you can also teach Dog B to withdraw in response to any noticeable warnings from Dog A, such as a hard stare or a lip curl. The advantage of a cue from Dog A is that it happens, and Dog B responds by leaving, even if you’re not there to give your cue.
Eventually you may find that the mere presence of Dog A-with-resource becomes the cue for Dog B to leave, which is just fine and dandy. If you see Dog B leaving the room before the cue, go ahead and reinforce that – it’s a good thing!
When the cue is given (yours, or Dog A’s), guide (lure or prompt) Dog B to a specified target, ideally in another room. Throw a treat-and-praise fest there for Dog B, and hang out with him there for several minutes before returning to Dog A’s room and repeating the process. Dog B should soon be dashing to the other room when the cue is given – either yours, or Dog A’s lip curl.
So what happens if Dog A is in the designated target room with a valuable resource? Great question! It’s a good idea to operantly condition Dog B to a second target location in a different room. When Dog A is in Room X, Dog B learns to target to the spot in Room Y. But if Dog A is in Room Y, Dog B learns to target to a spot in Room X.
Managing Resource Guarding in Dogs is an Ongoing Effort
Keep in mind that you are likely to always need some degree of management with resource guarding in dogs, even with your successful modification programs. For example, even if you’ve done a great job of modifying the behavior of a dog who tends to guard toys, the high-arousal of a dog-to-dog game of tug carries a high likelihood of retriggering guarding aggression. Reserve his tug playing for games with you, and limit his play time with his canine pals to romping and running games. Be smart. Manage as needed, keep your eyes open for signs of returning tension, and be prepared to do a little remedial modification as needed.
So there you have it. Select the method(s) that appeal to you to manage resource guarding in dogs and get started. It will do your heart good to see the decreasing tension between your canine family members. It will also be gratifying to see your guarder gain new associations and learn new behaviors without fear of losing his valuables to his four-legged siblings.
Thanks to Sarah Richardson, CPDT-KA, CDBC, of The Canine Connection in Chico, California, for modeling with Otto and Peanut.
The supply of Immiticide (melarsomine dihydrochloride), the only drug approved to treat heartworm infections in dogs, has been low since December 2009, but now it’s completely gone. Merial confirmed that it was officially out of the drug on August 9, 2011. The current situation is due to a new and separate manufacturing challenge related to technical issues with the company who provides the finished product, according to a Merial spokesperson. Merial said the company is working hard to make the drug available again, but cannot speculate when that might happen.
288
With Immiticide unavailable, the American Heartworm Society (AHS) has issued guidelines for treating heartworm-positive dogs to try to mitigate the damage that heartworms cause while in the body and the danger they present when they die. Briefly, here is what the AHS advises:
1) Verify all positive antigen tests with a second antigen test from a different manufacturer.
2) Give monthly heartworm preventive medication to prevent further infection. If the dog tests positive for microfilariae, pretreat with corticosteroids prior to giving the first dose of heartworm preventive medication and keep the dog under veterinary observation for at least 8 hours afterwards, due to the risk of anaphylactic shock from the rapid die-off of the microfilariae.
3) Treat dogs with doxycycline at the rate of 10 milligrams per kilogram of body weight twice a day for four weeks (give half as much if a dog cannot tolerate the higher dose). Repeat this dose quarterly (one month on, two months off) for as long as the dog is infected with heartworms. This will reduce the possibility of the infection being passed to other dogs through mosquitoes, shorten the lifespan of the adult worms, and lessen the chance of adverse side effects from worm death.
4) Restrict all activity and limit all exercise, as the danger from adult heartworms increases with physical activity.
5) Dogs with symptoms from the heartworms should receive medical treatment to alleviate respiratory distress. Surgical removal of the worms should be considered if cardiac function is affected.
6) When Immiticide becomes available, proceed with treatment if the dog still tests positive for heartworms.
I’d like to offer a few additional suggestions, based on what I’ve learned about this disease over the years.
While the AHS does not suggest any particular heartworm preventive medication, I recommend using Heartgard (ivermectin) or generic equivalent. Of the four drugs currently used to prevent heartworms, ivermectin has the strongest effect against adult worms. It also has a weaker effect against microfilariae, and so is unlikely to cause an adverse reaction, making pretreatment and observation less critical.
I also suggest giving weekly heartworm-preventive doses of ivermectin to most infected dogs. Be sure to use Heartgard, not Heartgard Plus or any other combination product, when giving weekly. Studies have shown that weekly ivermectin used along with pulsed doxycycline can reduce the number of adult heartworms by more than 78 percent over 36 weeks.
Do not combine Comfortis (spinosad), a newer flea-control product, with weekly doses of ivermectin, as it increases the risks of neurological side effects. Ivermectin should not be given more often than monthly to dogs with the MDR1 gene mutation making them more susceptible to certain drugs. Commonly affected breeds include the Australian Shepherd (standard and mini), Collie, Long-Haired Whippet, and Silken Windhound. See www.vetmed.wsu.edu/depts-VCPL for a list of affected breeds, and an inexpensive test to identify affected dogs.
As we discussed in “Update on Doxycycline and Heartworm Disease” (WDJ August 2009) and “Shortage of Immiticide for Heartworm Treatment” (April 2010), doxycycline is given to kill wolbachia, a symbiotic parasite that lives within heartworms. Destroying wolbachia weakens heartworms, makes them unable to reproduce viable offspring, reduces their adverse effects on the body, and decreases the likelihood of adverse reaction from their death. Doxycycline must be pulsed (given periodically) to keep wolbachia from repopulating. Studies that combined doxycycline with ivermectin for 36 weeks gave doxycycline during weeks 1 to 6, 10 to 11, 16 to 17, 22 to 25, and 28 to 33, but the schedule suggested by the AHS may be equally effective. Giving doxycycline with food can reduce gastric upset.
If Immiticide becomes available while your dog still tests positive for heartworms, you’ll have to decide whether treatment is warranted. Remember that the worms are doing damage as long as they are in the body, and danger of pulmonary embolism from their death also remains as long as any worms are present. Dogs showing symptoms of heartworm infection, those with heavy infections, and those who have been infected for a long time are most likely to benefit from Immiticide treatment, as are very active dogs, since the need for activity restriction would be shorter. Young heartworms are killed more quickly by the combination of ivermectin and doxycycline, so if the infection was caught early, later treatment with Immiticide is less likely to be needed. Keep in mind that dogs may test positive for heartworms for up to six months following the death of all worms.
If Immiticide treatment is not done, continue to give doxycycline quarterly until your dog tests negative for heartworms. Give ivermectin weekly to monthly while your dog remains infected.
For those considering natural heartworm treatment, remember that natural does not necessarily mean either safe or effective. These products are untested and usually contain toxic ingredients, such as wormwood (Artemisia absinthinium) and black walnut (Juglans nigra). The biggest danger of heartworm treatment is from the death of the worms, which can cause pulmonary embolism no matter how the worms die. There’s no reason to believe that alternative treatments are safer than conventional therapy, particularly if you do not give doxycycline as well.
– Mary Straus
For more information The American Heartworm Society: Guidance for Heartworm Disease Management During the Adulticide Unavailability
heartwormsociety.org/UrgentAlert-8-9-11.pdf
Heartworm Disease in Dogs: Prevention and Treatment
dogaware.com/health/heartworm.html
While treatment of Addison’s disease focuses on prescription drugs and electrolyte tests, holistic veterinarians add various support therapies to help their patients.
Standard Process
Nutrition is the cornerstone of every holistic therapy, and while diet cannot cure Addison’s disease, foods made of poor-quality ingredients or diets that lead to nutritional deficiencies are a significant source of stress, and additional stress is just what Addison’s dogs don’t need. Because wheat, corn, and soy are problem ingredients for some dogs, many holistic veterinarians recommend avoiding them. Some tell their clients to avoid grains altogether. In general, foods made from high-quality animal-source ingredients that are easy to digest work best, but because individual responses vary, caregivers should observe their pets’ responses and avoid ingredients that seem to trigger symptoms.
Veterinarians used to recommend adding salt to the food of dogs with Addison’s, but the benefits of the practice are not supported by research. Addison’s dogs do not require additional salt, which may lead to excessive thirst and urination.
The addition of probiotics can improve any dog’s diet, whether home-prepared, raw, cooked, canned, frozen, or packaged. Digestive enzyme powders are a sensible addition for any dog with digestive problems. These products are widely available in pet supply stores and online. Follow label directions.
Prior to the development of synthetic adrenal hormones, Addison’s disease was treated with glandular extracts. Adrenal cortical extracts given orally or injected are still available, though because synthetic versions have so thoroughly replaced them, few veterinarians are familiar with their use. Those who are often prescribe Standard Process Canine Adrenal Support, a powdered supplement that contains animal tissue extracts and other ingredients that support the adrenals. “The goal of Canine Adrenal Support,” explains the manufacturer, “is to help maintain the adrenal glands’ response to metabolic demand, normalize adrenal function, support the body’s ability to handle stress, and promote the adrenal glands’ ability to rebuild and regenerate.” Adrenal glandulars may reduce the amount of medication needed or just help the dog feel better, but their use requires close supervision from a knowledgeable veterinarian.
Some medicinal herbs are known for their effect on the adrenals. Six years ago, the New Zealand Veterinary Journal published a case report by R.H. Jerrett, et al, that examined the effect of whole, natural liquorice (Glycyrrhiza glabra – what we would call licorice) on a dog with Addison’s. The 4-year-old neutered male subject had persistently high potassium levels despite receiving a moderate dose of fludrocortisone. “Financial considerations and the potential for adverse effects made increasing the dose of fludrocortisone undesirable, so liquorice was added to the dog’s diet in hopes that the hyperkalemia would be corrected,” wrote the researchers. The dog’s potassium levels returned to normal, where they remained for the duration of the 14-month study. “Given these very preliminary findings,” the authors concluded, “we believe it is possible that liquorice may, in future, prove to be a useful adjunct in the management of canine hypoadrenocorticism.” It may also prolong the effect of corticosteroids.
Licorice is an adaptogenic herb, a category that describes medicinal plants that help the body deal with stress. Relaxing or sedative herbs help Addison’s patients, too. Oatstraw (Avena sativa) and German chamomile (Matricaria chamomilla) brewed as teas separately or together can be added to food or even applied to the skin and coat to help dogs feel relaxed. Other herbs may be beneficial for gastrointestinal upset and liver support.
Aromatherapy’s essential oils are more concentrated than herbal teas, so they should be diluted with vegetable oils before being applied to the skin, coat, or paw pads. For details see “Aromatherapy for Dogs,” WDJ 2004.
In her book, Holistic Aromatherapy for Animals, Kristen Leigh Bell describes her Calm Canine Essential Oil Blend, made with ½ fluid ounce (1 tablespoon) hazelnut, sweet almond, or other vegetable oil, 3 drops valerian (Valeriana officinalis), 2 drops vetiver (Vetivera zizanoides), 4 drops petitgrain (Citrus auranthium leaf), 3 drops sweet marjoram (Origanum morjorana), and 2 drops sweet orange (Citrus sinensis) essential oils. Combine and store in a dark glass bottle.
“This is my standard calming blend,” says Bell, “which has had a very impressive track record for dogs in numerous situations. The calming effect ranges from ‘taking the edge off’ to soothing a dog to the point where she gets very mellow and takes a nap.”
For best results use therapeutic-quality essential oils. Several pet aromatherapy companies make their own calming sprays and oils.
Melatonin, a hormone produced by the pineal gland, is sold as an over-the-counter supplement to help people with insomnia sleep through the night.
Veterinarians have found that when given to dogs, melatonin helps manage separation anxiety and fearful reactions to thunder, fireworks, and other noises. In other words, it helps reduce stress levels.
Melatonin is recommended (one 3-mg tablet or capsule for a medium-sized dog) 20 to 30 minutes before stressful events. Although some experts warn that melatonin may interfere with corticosteroids and other medications, others consider the benefits of occasional use to outweigh the risks. Consult your veterinarian as to whether melatonin is appropriate for your dog.
Calming pheromones provide stress relief, too. The product Comfort Zone contains “dog appeasing pheromone” (DAP), which may significantly reduce destructive behavior, fears, and phobias and help some dogs deal with stressful environments. Comfort Zone is sold in pet supply stores as a spray or with a plug-in electric diffuser.
Other techniques that help Addison’s dogs include massage, the playing of soft classical music, and energy therapies such as Reiki.
1. Become familiar with Addison’s symptoms so you can recognize them in a hurry.
2. If your dog shows symptoms, go to a veterinarian at once. Prompt treatment saves lives.
3. Learn about treatment options and cost-saving tips.
4. Schedule checkups and blood tests to monitor your dog’s condition.
5. Observe your dog’s behavior and appearance to help determine the ideal medication dosage for her.
Something’s wrong with your dog but you’re not sure what. She seems listless, her eyes have lost their spark, and she just seems “off.” You might notice intermittent muscle weakness, tremors, and an inability to jump into the car or onto a sofa. Or your dog frequently ignores her dinner, vomits, or has diarrhea. These vague symptoms, which may improve and then return, could stem from a dozen canine illnesses – or they might point to Addison’s.
Addison’s disease, named for the 19th century physician who defined this adrenal gland dysfunction, is also known as hypoadrenocorticism or adrenal insufficiency. Is Addison’s Disease fatal to dogs? Yes, if left untreated, but with appropriate treatment Addison’s can be managed so that affected patients lead normal, active lives. First diagnosed in dogs in the 1950s, it is considered an uncommon canine disorder. However, veterinarians who routinely test for Addison’s often find it, suggesting that the illness is not really rare but rather under-diagnosed and under-reported. You don’t find Addison’s unless you look for it. Some veterinarians speculate that Addison’s disease occurs in dogs at a rate as much as 100 times the rate in humans.
Aiyana, a three-year-old Italian Greyhound who lives with Lydia Kunzler in Northern Utah, developed symptoms when she was nine months old, but none of the several veterinarians Kunzler consulted could find the cause.
“Last fall I noticed Aiyana was starting to lose weight,” she says, “and because I had a lot of things going on I attributed her loss of appetite to stress and tried to feed her more. But a week after one of my other dogs passed away she became very sick. She was vomiting, very lethargic, and her digestive system just shut down, sometimes going days without a bowel movement. A few weeks went by, and we had to keep her on intravenous fluids or she’d get really sick again. Finally I decided to change vets. I knew all this vomiting, alternating diarrhea and constipation, and other symptoms weren’t normal.”
Aiyana’s new veterinarian immediately recognized the signs of Addison’s and did an ultrasound test, saw how small the dog’s adrenal glands were, and ordered an adrenal hormone blood test to confirm the diagnosis.
Recognizing Symptoms of Addison’s Disease in Dogs
Dogs of any breed, either sex, and any age can develop Addison’s. About 70 percent of dogs with Addison’s are female, although in some breeds, including Standard Poodles and Bearded Collies, males and females are equally affected. The median age of dogs diagnosed with Addison’s disease is 4 to 6 years, but it has been reported in puppies and in dogs as old as 12.
Certain breeds may be predisposed to Addison’s, including Portuguese Water Dogs, Bearded Collies, Standard Poodles, Great Danes, Soft Coated Wheaten Terriers, Airedale Terriers, Basset Hounds, Springer Spaniels, West Highland White Terriers, Leonbergers, Labrador Retrievers, Rottweilers, Saint Bernards, Nova Scotia Duck Tolling Retrievers, German Shepherds, German Shorthaired Pointers, other Poodles, and mixes of these breeds.
The most commonly reported symptoms of Addison’s disease, which can vary dramatically from dog to dog, include loss of appetite, weight loss, depression, listlessness, vomiting, diarrhea, hind-end pain, muscle weakness, tremors, shivering, increased thirst, excessive urination, a painful or sensitive abdomen, muscle or joint pain, and changes in coat, which may become thicker, thinner, longer, or even curly. About 15 to 20 percent of Addisonian dogs will have dark, tarry stools (melena, caused by gastrointestinal hemorrhage) or blood in their vomit. Symptoms often wax and wane, with the dog getting worse, then better, for months or even years.
Veterinarians examining Addison’s patients may notice mental depression, a thin or emaciated body, muscle weakness, dehydration, patches of darkened skin, a slow and weak pulse, low body temperature, low blood pressure, and pale mucous membranes. Blood tests may show any of the following: elevated potassium, low sodium, elevated BUN and creatinine, elevated liver enzymes, low glucose, high calcium, low protein (albumin and globulin), anemia, low cholesterol, and metabolic acidosis. Urine may be dilute (low specific gravity). A sodium/potassium ratio of less than 27 is strongly indicative of Addison’s, but a normal ratio does not rule it out, as many veterinarians assume. A sick dog with normal or elevated lymphocytes and eosinophils (lack of a stress leukogram) can point toward Addison’s.
Addison’s disease, called “The Great Pretender,” is often misdiagnosed because it resembles so many other illnesses. Both dog and human patients with Addison’s are often erroneously diagnosed as having gastrointestinal diseases such as inflammatory bowel disease (IBD), infections, parasites, cancer of the gastrointestinal tract, or poisoning. Acute renal failure, liver disease, urinary blockage, pancreatitis, insulinoma, hyperparathyroidism, and protein-losing enteropathy are other common misdiagnoses.
What is an Addisonian Crisis?
The most dramatic Addison’s symptom is the endocrine emergency called Addisonian crisis. This occurs when the dog goes into shock due to circulatory collapse, and it can happen so quickly that a healthy looking dog is suddenly, within a few hours, close to death.
In an Addisonian crisis, the lack of adrenal hormones depletes sodium levels (hyponatremia) and body fluids (hypovolemia), resulting in potassium retention (hyperkalemia), bradycardia (slow heart rate), hypotension (low blood pressure), associated cardiac arrhythmias (abnormal heart beats), and collapse. In other diseases, hypovolemia and shock cause tachycardia (rapid pulse); in Addison’s, the pulse slows. Low blood sugar levels (hypoglycemia) can cause seizures. Vomiting and diarrhea are common.
For many dog owners, the crisis is their first sign that something is wrong. About 30 to 35 percent of dogs with Addison’s are initially diagnosed during a crisis. Patients treated in time with intravenous fluid therapy and glucocorticoid steroids show such rapid improvement that it seems a miracle cure, though some have to be monitored and treated for several days before their condition stabilizes. And the cure is temporary, for without appropriate maintenance care, another crisis will follow.
As many as 90 percent of dogs in adrenal crisis will have elevated creatinine and BUN, which can lead to a misdiagnosis of acute renal failure. Dehydration and low blood pressure cause blood filtration to drop, resulting in “prerenal azotemia,” where waste products build up even though the kidney itself is functioning. Gastrointestinal bleeding can also cause increased BUN. The response to treatment is more dramatic for dogs with Addison’s disease than for those with kidney disease.
Addison’s Disease in Dogs: Types and Effects on the Body
The adrenals are two small glands positioned next to the kidneys. The center of each gland is called the medulla and the outer area is called the cortex.
The adrenal medulla secretes the “fight or flight” hormones: adrenaline (also called epinephrine) and noradrenaline (also called norepinephrine). These hormones are generally not affected by Addison’s disease, which affects only those secreted by the adrenal cortex: glucocorticoid and mineralocorticoid hormones. Addison’s can cause deficiencies of both types of steroid hormones.
Glucocorticoids (primarily cortisol) affect nearly every tissue in the body. They help maintain blood pressure and cardiovascular function, activate the body’s stress response, regulate metabolism and blood glucose levels, stimulate appetite, modify red and white blood cell production, and promote a general sense of well-being. Glucocorticoid levels are controlled by adrenocorticotropic hormone (ACTH), which is produced by the pituitary gland.
Mineralocorticoids (primarily aldosterone) are responsible for regulating electrolytes (sodium, potassium, and chloride) and water balance, which affects blood pressure. Electrolytes also affect nerve and muscle function, including heart rate and rhythm.
Typical Addison’s, often called primary Addison’s, is caused by adrenal dysfunction that creates both glucocorticoid and mineralocorticoid deficiencies. The adrenal glands atrophy, usually because of an autoimmune response that may be hereditary. Other possible causes include granulomatous disease, tumors, injury, prescription drug side effects, infection, or inflammation. By the time symptoms appear, an estimated 85 to 90 percent of the adrenal cortex has been destroyed. Dogs with typical Addison’s will have electrolyte imbalances, but this alone is not enough to diagnose the disease, nor can normal electrolytes rule out Addison’s disease.
In atypical Addison’s, the adrenal cortex continues to produce aldosterone but not cortisol. Patients with atypical Addison’s have normal sodium and potassium levels. Most eventually progress to typical Addison’s disease within a few months or, in some cases, years.
In secondary Addison’s, the pituitary gland no longer produces ACTH because of immune-mediated damage, inflammation, trauma, or cancer. Similar to atypical Addison’s, only cortisol production is affected, but secondary Addison’s will never progress to the typical form of the disease. Because aldosterone is still produced by the adrenal cortex, secondary Addison’s disease does not cause electrolyte imbalances.
What Causes Addison’s Disease in Dogs?
Addison’s disease can be brought on by treatment for Cushing’s disease designed to suppress or destroy overactive adrenal glands. The antifungal medication ketoconazole is sometimes used to treat Cushing’s because it suppresses adrenal function. The sudden withdrawal of prednisone or other cortisone medications after long-term use can also trigger an Addisonian crisis.
The Addison’s Disease Diagnosis
The ACTH (adrenocorticotropic hormone) response (or stimulation) test is considered definitive for Addison’s. Dogs must be off all corticosteroid hormones except dexamethasone for at least 12 to 36 hours (or more, if they’ve been on steroids for a long time) to prevent the drugs from affecting test results.
The cortisol level of an initial blood sample is measured; then the dog is injected with a form of the pituitary hormone ACTH that signals the adrenals to produce cortisol. One hour later, the blood cortisol level is measured again. In healthy dogs, cortisol levels rise, indicating a normal adrenal response. If the dog’s initial cortisol level is low and there is little or no response after ACTH stimulation, the diagnosis is Addison’s disease.
Synthetic ACTH (cosyntropin, Cortrosyn) is preferred for consistency; ACTH gels are not recommended for this test, because the results may not be accurate. An older protocol used one vial (250 mcg) of Cortrosyn for every dog, but only 5 mcg/kg is needed to achieve maximal adrenal stimulation when given intravenously. This can translate into a substantial cost saving for small dogs.
If the ACTH response test is positive and electrolytes are normal, then a separate test to measure endogenous ACTH levels can differentiate between primary and secondary Addison’s. Endogenous ACTH levels will be greatly elevated with primary Addison’s but low or undetectable with secondary Addison’s. Dogs with secondary Addison’s will never develop electrolyte abnormalities, making treatment and monitoring much less expensive.
Two situations can result in a misdiagnosis of Addison’s disease. Dogs from breeds originating around the Pacific Rim, including the Akita, Shiba Inu, and Jindo, often have elevated potassium values. This can be confused with Addison’s, particularly when symptoms are similar.
Whipworms can create a syndrome nearly identical to Addison’s, including low sodium and elevated potassium. Fecal tests for whipworms are often negative because eggs are shed infrequently.
In both cases, ACTH response tests will be normal. Always confirm a diagnosis of Addison’s disease before beginning mineralocorticoid supplementation.
Addison’s Disease Treatment for Dogs
In an Addisonian crisis, treatment with intravenous fluids, glucocorticoids such as dexamethasone, and sometimes glucose as well can literally save a dog’s life. Once the patient’s condition has stabilized, treatment moves to the life-long replacement of adrenal hormones, along with careful monitoring of electrolyte levels for dogs with typical Addison’s.
Glucocorticoid hormones such as prednisone, prednisolone, methyl-prednisolone (Medrol), or hydrocortisone are needed for all dogs with Addison’s disease. For atypical and secondary Addison’s, this is the only drug prescribed. Prednisolone and methylprednisolone have been converted to a bioactive form, a process which otherwise must be done by the liver, so these may be good choices for dogs with elevated liver enzymes. Methylprednisolone and hydrocortisone may be associated with fewer side effects. Hydrocortisone is synthetic cortisol, closest to the natural form.
The starting dose is 0.1 to 0.2 mg prednisone (0.4 to 0.8 mg hydrocortisone) per pound of body weight daily. This is a physiologic dose, meant to mimic the amount of cortisol the body would produce itself if it were able. It should not cause the type of side effects associated with prednisone given at therapeutic levels for dogs with problems such as allergies or autoimmune disorders.
Many dogs do well on 0.05 mg prednisone (0.04 mg Medrol, 0.2 mg hydrocortisone) per pound of body weight daily. Even large dogs usually do not require more than 5 mg daily, except during times of stress. The dosage is best divided in half and given every 12 hours in order to keep cortisol levels more even, particularly when using hydrocortisone, which has a much shorter half-life.
Dogs with typical Addison’s also need mineralocorticoid supplementation. Two options are available: fludrocortisone acetate (Florinef) and desoxycorticosterone pivalate (DOCP, commonly known by the brand name Percorten-V).
Florinef is an oral medication that is given once a day in the morning or split into two daily doses. Missing even a single dose can be dangerous. It can be difficult to regulate dogs taking Florinef, and increases in the initial dosage are frequently required, especially during the first year, as any remaining adrenal function is lost.
Percorten for Dogs
Percorten-V is given by subcutaneous injection once every 25 days or so. Experts find that in addition to having fewer side effects, Percorten-V regulates electrolytes more effectively than Florinef. Dogs who have problems when taking Florinef, including excessive thirst, urination, or incontinence, may do better with Percorten-V.
Aiyana, the Italian Greyhound who was finally diagnosed with Addison’s disease, was initially treated with Florinef. “Her electrolytes wouldn’t stabilize, and she didn’t respond as expected,” says Kunzler. “My vet switched her to Percorten-V injections, which has made a lot of difference.”
Dogs on Percorten-V require glucocorticoid supplements, such as prednisone, in addition to their monthly injections. Fludrocortisone has some glucocorticoid activity, so about half of the dogs who take this medication do not require regular glucocorticoid supplements, and others may need supplements every two or three days rather than daily.
All dogs with Addison’s need additional glucocorticoids during times of stress, injury, or illness. What constitutes stress will vary from one dog to another. Stress can be physiological, such as a medical procedure, injury, or even a particularly active play session. Stress can also be emotional, such as from a move, the loss of a human or animal companion, thunderstorms, fireworks, a visit to the vet’s office, or anything that disrupts familiar routines.
Stress increases the need for glucocorticoids from two to four times the maintenance level. A dog undergoing surgery may need even more, starting with a high dose and quickly tapering back to normal during the following week. An alternative would be to give an injection of dexamethasone during surgery, followed by oral steroids after. Fluid support should always be provided for Addisonian dogs during surgery.
Canine Addison’s Disease Life Expectancy and Management
With appropriate treatment, dogs with Addison’s share an excellent prognosis, with no anticipated disease-related problems affecting their life expectancy. Dogs usually feel better within days of starting treatment, and most symptoms are gone within two to four weeks. The main challenges to life-long treatment are its expense and the effort involved in monitoring electrolyte levels, administering medication, and keeping a close eye on the patient for signs of problems.
It’s important to monitor electrolytes through regular blood tests, especially when treatment begins. With Florinef, blood tests are initially done weekly, then gradually decreased once electrolytes reach normal levels, with continued monitoring two to four times a year after the dosage has stabilized. Dogs receiving Percorten-V are tested before each injection as the dosage is tapered to the lowest level needed, and then tested at least once or twice a year thereafter. Electrolytes should also be tested whenever the dog seems “off.” Dogs with atypical Addison’s require monitoring as well, in case the disease progresses to the typical form.
Dehydration or elevated potassium is indicative that the dosage may be too low. Dehydration causes tacky gums or shoulder skin that doesn’t snap back when pinched. Elevated potassium levels may slow the heart rate – a normal pulse for large dogs ranges from 60 to 100 beats per minute, and for smaller dogs 100 to 160 beats per minute. Severe muscle weakness may be due to low potassium from a dosage that is too high. Symptom changes should be reported as soon as they occur so that medication can be adjusted.
Cortisol levels are monitored not through blood tests but by observation of behavior. The goal is to give the lowest dose of glucocorticoids needed to keep your dog symptom-free, eating well, and happy.
Symptoms such as excessive thirst and urination, ravenous appetite, panting, hair loss, muscle atrophy, elevated liver enzymes, and frequent infections are indications that the glucocorticoid dosage is too high. Lack of appetite or energy, vomiting, diarrhea, and weakness or lethargy indicate that the dosage may be too low. Similar problems may be seen with too much or too little Florinef.
Zala Bu, a five-year-old Great Dane who lives with Jenny Schultz of Denver, North Carolina, was diagnosed with Addison’s at 18 months. “Her previous family did not follow up with their vet by doing continual blood testing to monitor her progress,” says Schultz. “To add to that, their vet was not prescribing a high-enough dose of Florinef, her first medication. As a result, Zala’s health declined. She came to me as a foster dog when she was in her second crisis and her family was fed up with dealing with her illness. She was anorexic, vomited frequently, and had chronic diarrhea. She had lost 30 pounds in six months.”
Schultz changed Zala’s medication to Percorten-V, which she says is “by far our preferred choice as it keeps the dog’s electrolytes consistent throughout the month and helps get a dog back to good health much faster.
“Her life started over the day she joined my pack,” she says. “Zala has been healthy for three years now and is a very active Dane. She takes an extremely low dose of Percorten-V as a shot that I give her at home, along with 1 mg prednisone daily. She gets her electrolytes checked every two to three months at the vet’s office to make sure the medicine is working well and that her electrolytes are balanced. Zala Bu started on 2.8 ml of Percorten-V and I have tapered her down to a .9‑ml dose.”
According to Schultz, a big challenge after an Addison’s diagnosis is to find a veterinarian who is willing to fine-tune the dog’s medication. “When dogs are at their lowest effective dose, they feel their best,” she says. “There are still many vets who don’t know how to treat this disease. As a result, dogs in their care are not as healthy as they could be.”
If problems continue after electrolytes are stabilized and the appropriate glucocorticoid dose is determined, consider other concurrent causes, such as liver disease, spay incontinence, or gastrointestinal disease. Dogs with Addison’s may be particularly prone to other autoimmune diseases such as hypothyroidism.
Jenn, a chocolate Labrador Retriever belonging to Margaret Daunt of Modena, New York, developed typical Addison’s 10 years ago at age 4. One year later she was diagnosed with hypothyroidism. At age 13 she survived bloat (“I believe quick action on my part saved her life,” says Daunt), and earlier this year, she was diagnosed with the tick-borne disease ehrlichiosis.
“Jenn has led an active life,” says Daunt. “She competed in agility, trained in obedience, and even dabbled in drug detection work. Now that she has recovered from ehrlichiosis, 14-year-old Jenn is back to her old self!”
It’s important to be alert, as Daunt was, to all symptoms of Addison’s disease in dogs. Don’t assume that every time your dog doesn’t feel well it must be due to Addison’s disease. Addison’s dogs develop illnesses just as other dogs do. If an Addison’s dog is sick from something else, her prednisone dosage may need to be increased temporarily.
Your Dog’s Addison’s Disease Treatment Costs
To make Addison’s treatment affordable, many caregivers purchase compounded fludrocortisone from a compounding pharmacy. “The compounded version is much more cost-effective for larger dogs than brand-name Florinef,” says Schultz, who participates in online forums for canine Addison’s. Most dogs who receive Percorten-V injections and about half of those who take Florinef require a small daily oral dose of inexpensive prednisone as well.
The online Addison’s groups share information about the disease and suggestions for reducing costs. “Our FaceBook and Yahoo groups help people understand lab test results and talk to their veterinarians about adjusting medications,” says Schultz. “We also help people find lower-cost options for treating their pets. In some cases owners were able to keep their pets when they couldn’t afford the prices their vets were charging. One single mom was paying $300 per month for her Great Dane’s shots until she switched to compounded medications that cost only $30 per month. Two years later, her Dane is still with her and doing well.”
Other money-saving strategies include giving shots at home to avoid having to pay for an office visit for each injection, purchasing medications online at a discount with the help of veterinarians willing to write the necessary prescriptions, or negotiating with veterinarians to keep office visit costs to a minimum. Schultz estimates her monthly expenses at $35 for Percorten-V and another $25 for electrolyte tests. “We test Zala Bu every other month now because we’re adjusting her dose downward,” she says. “She is small for a Dane, weighing in at 102 pounds. I get a large script for prednisone filled at a pharmacy for $4. Zala Bu is the poster child for low-dose effectiveness in big dogs.”
Elizabeth Andrews of Pleasantville, Nova Scotia, Canada, joined the online group AddisonDogs in 2006, when Raider, her 75-pound Labrador Retriever, was diagnosed with typical Addison’s. Raider is now six years old and thriving, and Andrews is a list moderator. “The AddisonDogs group was founded in 2002 and currently has 4,594 members,” she says. “We also run a 501(c)(3) non-profit organization called AddisonDogs to educate and support the companion animal community about this condition, and the AddisonDogs website helps re-home dogs with Addison’s disease and assists with vet bills and other expenses. I am also the owner of a FaceBook Group, Addison’s Disease in Dogs, which has 559 members and is growing daily.”
Andrews explains that in the U.S., brand-name Florinef costs about $1 per 0.1-mg tablet, and the minimum starting dose is 0.1 mg per 10 pounds of body weight with dogs normally needing two to three times the starting dose. In Canada, Florinef costs about 27 cents per tablet when purchased at a drugstore. Florinef can also be purchased in the U.S. from compounding pharmacies, which reduces the total monthly cost regardless of dose to about $30.
Percorten-V purchased online costs $150 to $190 per vial depending on the supplier. “Most AddisonDogs members buy it for $150 from the online pharmacy 1-800-PetMeds,” says Andrews, “because that company price-matches the lowest price online. However, many veterinarians in the U.S. refuse to give their clients a prescription for Percorten-V, arguing that the drug sold online may be counterfeit. A few vets will price-match. Veterinarians pay approximately $130 U.S. for a 4-ml (100-mg) multi-use vial directly from the manufacturer, Novartis, but this life-saving drug often has a high retail markup.”
The typical starting dose of Percorten‑V is 1 mg per pound of body weight. Dr. David Bruyette, DVM, DACVIM, of VCA West Los Angeles Animal Hospital and an internal medicine specialist with an emphasis on Addison’s disease, prefers to start large dogs (over 60 pounds) at half that amount, because their metabolism is slower. He points out that electrolytes should be measured more frequently when using a lower starting dose; he recommends checking at two, three, and four weeks after the first injection.
Julia Bates, DVM, of Veterinary Specialty & Emergency Care in Madison, Wisconsin, is a veterinary internist whose research during her residency involved the use of low-dose Percorten-V in the management of Addisons disease. She routinely treats dogs diagnosed with Addison’s disease with a low dose of Percorten-V. In her experience, the majority of those dogs do very well.
Ideally, the dose is gradually tapered down until the lowest effective dose is found. “We know that lowering the dose works,” says Andrews, “as many in our Yahoo group have been doing so for over five years.”
As mentioned, dogs should be monitored while their drug dosages are being adjusted. “With Percorten-V, blood electrolytes should be tested at day 14 and then at day 25,” says Andrews. “The day-14 electrolytes show how well the Percorten-V is working, and the day-25 electrolytes show whether the dog will be ready at day 28 for more Percorten-V and whether the dose can be reduced. It is very common for a dog not to be ready for more during the first few months. Giving more Percorten-V before the dog is ready just drives potassium levels down. By waiting for potassium levels to rise and then reducing the dose, you ‘balance’ the electrolytes. Once the lowest effective dose has been found, you can test electrolytes every six months or whenever the dog’s behavior or symptoms seem different.”
Adjusting patients to Florinef requires much closer monitoring of electrolyte levels. “It’s important to test weekly until they stabilize,” says Andrews. “Most dogs need their dose increased frequently over the first few weeks and months. Once you find a dose that maintains stable electrolytes for a few weeks, you can move to biweekly testing and then monthly tests. After an effective dose has been found, testing every three months is recommended for life. Of course not everyone does this, and those who don’t generally end up having a dog go into crisis.”
Managing Stress for a Normal Life with Addison’s Disease
All the experts agree that a properly treated dog can live a normal, happy, healthy life despite having Addison’s disease.
“Since stress can be an issue for dogs with Addison’s,” says Jenny Schultz, “caregivers may have to cut back on stressful activities depending on their dogs’ temperament. My Great Dane used to make therapy dog visits to a nursing home. She enjoyed the activity and it didn’t seem to stress her too much. A little extra prednisone as a boost and a good nap was all she needed to continue on with her day. She is by far the most active dog in our pack. Some dogs with Addison’s continue to compete in agility and obedience events with no problem after their condition has been stabilized.”
In her book, Addison’s Disease in Dogs, Stephanie Kenrose describes the importance of long-term stress management and supplying extra prednisone whenever an Addison’s dog is stressed by injury, trauma, illness, or other events. She also discusses the stress created by annual vaccinations and heartworm prevention medications, noting that titer tests can be used to monitor immunity to common canine illnesses, and decisions about heartworm prevention depend on one’s location as well as the dog’s condition. “You’ll want to discuss these risk factors with your veterinarian,” she says, “so that you can decide whether it’s worth giving these medicines to your Addison’s dog.”
After eight months of treatment, Aiyana, the Italian Greyhound, is doing much better. “She was spayed just three weeks ago,” says Lydia Kunzler, “which caused her Addison’s to flare and her electrolytes to go a bit off again, but she was much easier to stabilize this time. The blood work we took last Wednesday was the best it’s been since she was first tested!
“She still struggles with muscle weakness especially in her rear from time to time, and she needs a little extra prednisone some days, but getting her spayed so those hormones weren’t complicating things seems to have made a big difference. I’ve also stopped feeding any dry food, per my vet’s advice, as we were having a hard time maintaining her hydration levels. She mainly eats raw now, or canned food if I’m going to be traveling, and I feed her three to four small meals a day instead of two big meals to make it easier on her GI system.”
Caring for a dog with Addison’s disease can seem overwhelming at first, both financially and emotionally. But properly treated, your Addisonian dog can live just as long and just as well as her disease-free counterparts.
Freelance writer CJ Puotinen lives in Montana. She is the author of The Encyclopedia of Natural Pet Care, and other books, and is a frequent contributor to WDJ.
Mary Straus is the owner of DogAware.com. She and her Norwich Terrier, Ella, live in the San Francisco Bay Area.
On occasion, an adult dog who has been trustworthy with his chewing habits may suddenly surprise you with an oral foray into the forbidden.
This may be a stress response to something environmental happening in your absence, such as a burglar trying to break into your home, loud equipment working in the street in front of your house, or stray dogs romping through your yard. Sometimes even something like a compelling need to urinate or defecate can stress a well-trained dog into inappropriate chewing.
If you can determine the nature of the stressor and control or remove the cause, your dog should quickly revert to his prior good chewing behavior. He might also need a refresher course in the crate, after a veterinary exam to rule out possible medical causes. (Anytime there’s a significant behavior change in an adult dog it’s important to rule out – or treat – any possible medical contributors to the undesirable behavior.)
A return to inappropriate chewing may be a result of inactivity and pent-up energy. Perhaps the weather’s been bad or your workload extra heavy, curtailing your normal exercise sessions with your canine companion. That energy has to go somewhere – and for some dogs, it goes right to their jaws. The solution here is a renewed commitment to provide adequate exercise, with the addition, perhaps, of mental exercise into your dog’s daily routine.
To provide the best experiences, we use technologies like cookies to store and/or access device information. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.
This website uses cookies and other tracking technologies to offer you a better experience, personalize content and ads, and analyze our site traffic. Before proceeding, you agree to our Terms and that you’ve read our Privacy Policy. Update Settings
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.